The Diabetic Foot – How to save a limb
by Kevin Cassar
The high prevalence of diabetes mellitus in our country is well recognized and it is estimated that there are around 40,000 diabetics in Malta. This is steadily increasing, as it is in the rest of the world, as a result of longer life expectancy, sedentary lifestyles, and dietary choices. Diabetic foot problems are the most serious and costly complications of diabetes. The World Health Organisation estimates that in the high income countries treatment of diabetic foot complications accounts for 15-25% of all healthcare resources for diabetes. Over 1 million major lower limb amputations are performed each year in diabetics amounting to a leg being lost to diabetes every 30 seconds. In Malta 120 major amputations are performed per year and this figure has remained relatively static for at least the last 6 years. The sad thing is that a lot of these complications can be prevented using low cost and low technology solutions. The International Working Group on the diabetic Foot (IWGDF) states that by implementing a care strategy that combines prevention, the multidisciplinary treatment of foot ulcers, appropriate organization, and close monitoring and education of people with diabetes and healthcare professionals, it is possible to reduce major amputations by a staggering 85%!
What causes diabetic foot problems?
Foot problems arise mainly because of one or both of the following conditions: peripheral neuropathy and/or peripheral vascular disease. Peripheral neuropathy causes loss of sensation, autonomic dysfunction and alteration of the shape of the foot which predisposes to the development of ulceration, diabetic foot infection, and Charcot’s osteoarthropathy. The prevalence of polyneuropathy in diabetics is estimated to be around 24% in Type II diabetics.1
Diabetes is a major risk factor for atherosclerosis and as a result many diabetics suffer from peripheral vascular disease affecting any part of the vascular tree including the aortoiliac segments, the femoropopliteal segment and the crural vessels. Based on UK population surveys peripheral vascular disease occurs in up to 23% of diabetics.2 Although diabetics also suffer from microangiopathy, the major problem with diabetics who have arterial disease lies in the major arteries. It is a commonly held misconception that there is nothing to do for diabetics with arterial disease because the problem lies in the small vessels. Nothing could be further from the truth. Most diabetics with arterial disease are amenable to revascularisation either using endovascular or open surgical techniques. There is clear evidence that with increasing numbers of revascularisation there is a drop in the number of major amputations performed.3-5
In the vast majority of diabetic patients who end up requiring a major amputation, there is a repetitive causal sequence of minor trauma, ulceration and wound healing failure which often goes on for several weeks if not months.6 Based on the recognition of the sequence of events, various guidelines have been drawn up for Diabetic Foot Care including SIGN (Scottish Intercollegiate Guidelines Network guideline 55), NICE guidance (National Institute of Clinical Excellence), and the Consensus statement of the International Working Group for the Diabetic Foot. All of these guidelines have a common theme – that a significant proportion of major amputations can be prevented if adequate measures are in place.
How can amputations be prevented?
Education
Footcare education is a fundamental part of the strategy to save limbs in this group of patients. There is evidence that programmes which include education with podiatry show a positive effect on minor foot problems within a relatively short space of time.7,8 A randomized controlled trial showed that by showing diabetic patients the potential complications of diabetic foot disease, amputations and recurrent ulceration were prevented.9
Foot Screening
Because of the high prevalence of neuropathy in this group of patients a lot of them are asymptomatic even when they have severe ischaemia or ulceration. As a result pain cannot be relied upon as a symptom in this cohort. It is therefore recommended that all diabetics undergo foot screening.
Foot screening should involve:
- assessment of sensation by using clinical neuropathy scores or 10g
microfilaments or vibration sensation perception threshold;
- examination of pulses;
iii. inspection of the feet for deformity, ulceration, callus, and inspection of footwear.
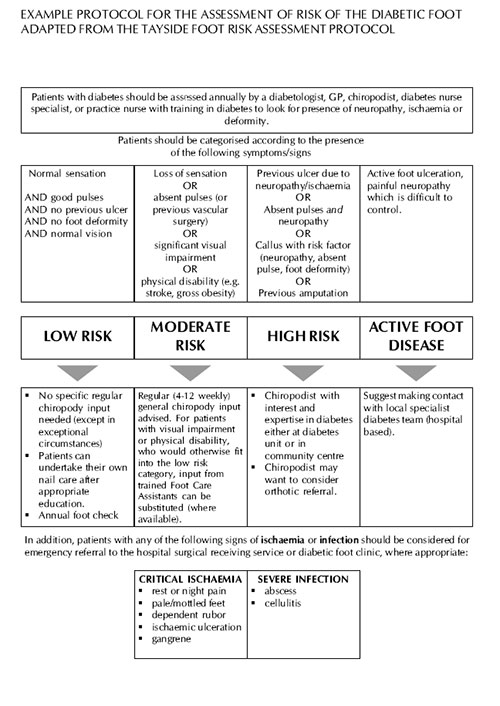
There is no agreed frequency for foot screening but NICE guidance recommends that annual review should be arranged at which, based on the observations made, patients are stratified into risk groups for foot ulceration: low, medium and high risk or in those who have already developed ulceration or tissue loss as ‘ulcerated foot’.
Classification into these groups is based on standard criteria and action is initiated based on the classification group (Figure 1). This screening ensures that those at high risk in particular are seen regularly and active measures are taken to reduce the risk of development of ulceration to the minimum possible. More importantly, those who have ulcers or gangrene should be referred immediately to hospital. Patients with new ulceration, swelling and discoloration should be seen in hospital within 24 hours. The reason is that in this situation the damage sustained by the foot can progress very rapidly. Any delay in appropriate referral of these patients will inevitably lead to limb loss.
Structured foot care
There is level I evidence that access to podiatry reduces the number and size of foot calluses and improves self care.7 A multidisciplinary foot team has been shown to allow rapid access to vascular surgery and intensive treatment, including control of infection and revascularisation which leads to wound healing and foot saving amputations which ultimately leads to a reduction in the number of major amputations.10 All patients with diabetes should have access to structured foot care.
Footwear, Orthoses and Total contact casting
Ordinary shoes should be avoided in diabetics as plantar pressures generated using normal footwear is equivalent to walking barefoot. These patients should be advised at least to wear high quality cushioned-soled trainers.11,12 These however are not as effective as custom built shoes in reducing plantar pressures and therefore the risk of ulceration.13,14 Access to total contact casting is important both for the treatment of acute Charcot’s osteoarthropathy and in the treatment of neuropathic ulceration.15
Arterial reconstruction
The identification of an ulcer in a diabetic does not constitute a diagnosis. An ulcer is simply a clinical sign of an underlying problem which in diabetics is either neuropathy or arterial disease or both. In the case of arterial disease, in the majority of cases this can be treated. It is therefore crucial that patients with ulceration are referred as early as possible. There is little point in treating these patients with repeated applications of the local favourite topical antibiotic or oral antibiotics in increasing doses and combinations or prescribing increasingly expensive and fancy local dressings. Identification of arterial disease requires initiation of treatment to control risk factors – diabetes control, treatment of hypertension, initiation of antiplatelet treatment and statins, and smoking cessation. If the patient’s foot is ischaemic the solution is to refer quickly for revascularisation. Indeed failure to feel bounding and easily palpable pulses in these patients should instigate an immediate referral for vascular assessment. If no pulses are felt one should assume that the ulcer is ischaemic until proven otherwise through a full vascular assessment. Rates of limb salvage after distal bypass surgery are relatively high with salvage rates of over 80% reported in the initial presence of tissue loss or gangrene.5
References
- Young MJ, Boulton AJM, McLeod AF et al. A multicenter study of the prevalence of diabetic peripheral neuropathy in the United Kingdom hospital clinic population. Diabetologica 1993; 36:150-4
- 302 Williams and Airey, 2000 The size of the problem: Epidemiological and economic aspects of foot problems in diabetes In “The Foot in diabetes” 3rd ed. Boulton, AJM, Connor, H, Cavanagh, PR (Eds.) John Wiley & Sons, Chicester.
3.Conte MS, Belkin M, Upchurch GR, Mannick JA, Whittemore AD, Donaldson MC. Impact of increasing comorbidity on infrainguinal reconstruction: a 20-year perspective. Ann Surg 2001; 233: 445-52.
4.Shah DM, Darling RC 3rd, Chang BB, Fitzgerald KM, Paty PS, Leather RP. Long-term results of in situ saphenous vein bypass. Analysis of 2058 cases. Ann Surg 1995; 222: 438-46.
5.LoGerfo FW, Gibbons GW, Pomposelli FB, Campbell DR, Miller A, Freeman DV, et al. Trends in the care of the diabetic foot. Expanded role of arterial reconstruction. Arch Surg 1992; 127: 617-21.
6.Pecoraro RE, Geiber GE, Burgess EM. Pathways to diabetic limb amputation: basis for prevention. Diabetes Care 1990; 13: 513
7.Rönnemaa T, Hamalainen H, Toikka T, Liukkonen I. Evaluation of the impact of podiatrist care in the primary prevention of foot problems in diabetic subjects. Diabetes Care 1997; 20: 1833-7.
8.Dargis V, Pantelejeva O, Jonushaite A, Vileikyte L, Boulton AJ. Benefits of a multidisciplinary approach in the management of recurrent diabetic foot ulceration in Lithuania: a prospective study. Diabetes Care 1999; 22: 1428-31.
- Malone JM, Snyder M, Anderson G, Bernhard VM, Holloway GA Jr, Bunt TJ. Prevention of amputation by diabetic education. Am J Surg 1989; 158: 520-3
- Faglia E, Favales F, Aldeghi A, Calia P, Quarantiello A, Barbano P, et al. Change in major amputation rate in a center dedicated to diabetic foot care during the 1980s: prognostic determinants for major amputation. J Diabetes Complications 1998; 12: 96-102
11.Kastenbauer T, Sokol G, Auinger M, Irsigler K. Running shoes for relief of plantar pressure in diabetic patients. Diab Med 1998; 15: 518-22.
12.Perry JE, Ulbrecht JS, Derr JA, Cavanagh PR. The use of running shoes to reduce plantar pressures in patients who have diabetes. J Bone Joint Surg Am 1995;
- Uccioli LE, Faglia, Monticone G, Favales F, Durola L, Aldeghi A, et al. Manufactured shoes in the prevention of diabetic foot ulcers. Diabetes Care 1995; 18: 1376-8.
14.Colagiuri S, Marsden LL, Naidu V, Taylor L. The use of orthotic devices to correct plantar callus in people with diabetes. Diabetes Res Clin Pract 1995; 28: 29-34.
15.McGill M, Molyneux L, Bolton T, Ioannou K, Uren R, Yue DK. Response of Charcot’s arthropathy to contact casting: assessment by quantitative techniques. Diabetologia 2000; 43: 481-4.
Figure 1: Adopted from SIGN guideline 55.