
New Developments in Breast Cancer Detection
by Pierre Vassallo – Imaging options for breast cancer detection have changed significantly over time. There are two goals that drive technological change in breast cancer imaging: a. improvement in diagnostic accuracy and b. reduction in radiation exposure to the breast.
The gold standard for breast cancer detection has long been the standard two-plane mammogram; this was initially obtained using conventional film/screen technology and later with full field digital mammography (FFDM), which improved image quality and reduced radiation exposure.
Digital breast tomosynthesis (DBT) integrates tomography into digital mammographic technology. This imaging method obtains multiple slices through the thickness of the breast thereby reducing interference from tissue overlap, which is particularly advantageous in dense breasts. The current practice is to start with FFDM as the initial screening test and to proceed to DBT only if questionable findings are noted on FFDM.
From a cancer detection standpoint, combining FFDM and DBT improves cancer detection rates (CDR), however this also leads to doubling in radiation dose delivered to the breast. Performing DBT alone is not recommended as it involves longer reading times and does not deliver the initial overview of the breasts provided by FFDM, which greatly aids cancer detection.
Recent technological development in DBT has led to synthesised views (or S-views), which are single mammographic images created from the DBT data. An S-view image is similar to an FFDM mammogram. Using DBT/S-views reduces the radiation dose by 50% compared with FFDM/DBT combined. DBT with S-views may therefore be used as a primary cancer screening exam to replace FFDM/DBT.
Current scientific literature analysing over 30,000 screening exams has shown an improved CDR with DBT/S-views (9.3 per 1000 screening exams) compared with FFDM (5.4 per 1000 screening exams); the relative (detection) rate (RR) is 1.72. Using DBT/S-view improves CDR irrespective of breast density, but the benefit is greater for dense breasts; RR for is 2.86 for high density breasts and 1.52 for low density breasts. The positive predictive value (PPV), which is the proportion of correct positive diagnoses, using DBT/S-view (23.3%) is double that of FFDM (12.9%) (Caumo, et al., 2017).
An important criterion for assessing a screening test is the recall rate; since mammograms are taken in the absence of a radiologist in most screening programs, patients need to be recalled for further investigation if the radiologist detects an abnormality. A very high recall rate is associated with significant distress and expense, since many of the recalled patients will not have cancer. A low recall rate, however, may miss cancers. The recall rate for DBT/S-view is similar to FFDM.
The review time required by the radiologist for DBT/S-view is however almost double that of FFDM.
Similar results were obtained in earlier studies from different research groups (Holt, et al., 2017); they described significant reduction in radiation dose using DBT/S-view technology compared with DBT/FFDM combination.
Tomography uses a long-known principle that acquires a slice image through the body by moving the X-ray source and detector during the image acquisition (Figure 1). This movement retains in focus those structures that are at the focal point of rotation, while blurring all structure in front of and behind that plane of focus. The use of tomography started in the 1930s and was enhanced in the late 1960s and 1970s with the development of powerful computers that could handle large volumes of data fast. These technologies gave rise to Computed Tomography (CT), which is one of our most powerful diagnostic tools.
Integration of tomography into breast imaging was suggested in the late 1990s, however prototype systems that were developed were not practical due to limited detector technology and computing power. With the improvement of x-ray detectors and computing power, DBT systems have been increasingly introduced into clinical use over the past decade (Figure 2).
DBT has been used to evaluate complex and equivocal findings as part of a diagnostic mammographic imaging work-up (Figures 3 and 4), but its implementation for breast cancer screening was hindered due to increased radiation exposure it entails.
By employing the latest development in DBT, namely the S-view, the radiation exposure is reduced to by half, which makes it acceptable for use in breast cancer screening. The diagnostic accuracy of the DBT/S-view is higher than that of the standard FFDM/DBT combination (Figure 5) according to the latest research (Caumo, et al., 2017).
Breast cancer is the most common cancer in women account for around 50% of all female cancers. The frequency of breast cancer and the availability effective treatment justify regular screening for all women particularly those who have risk factors. The dense breast is one of the limitations of mammographic imaging and is also a risk factor for breast cancer. The S-view technology provides a more accurate and safe method of screening for breast cancer than was previously possible. This is particularly true when evaluating dense breasts.
Figure Legends:
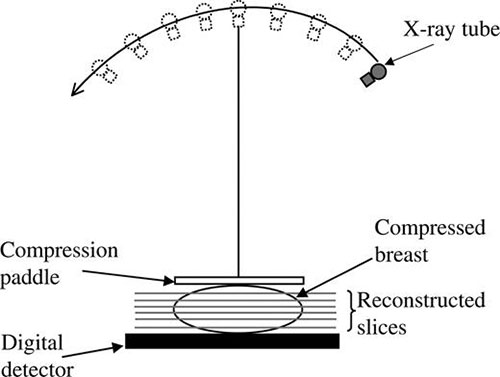
Figure 1: Diagram showing movement of X-ray source to obtain slice images through the breast.
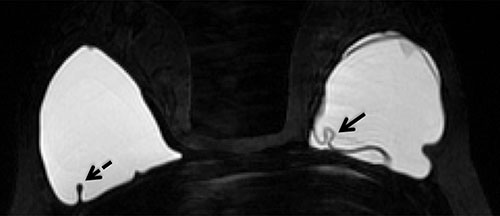
Figure 2: Clinical implementation of DBT.
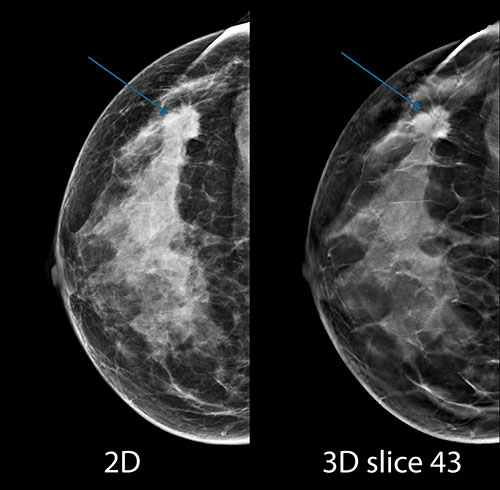
Figure 3: FFDM (Left) and DBT (Right) showing a cancer (arrows) in the lateral aspect of the left breast.
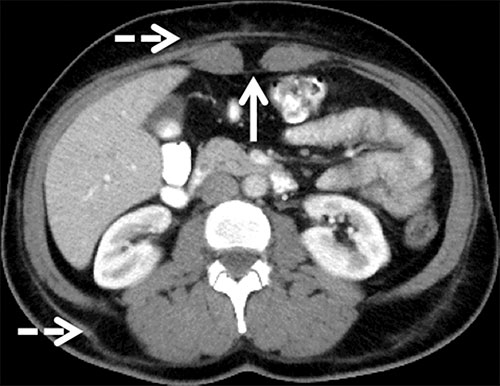
Figure 4: Zoomed image of a cancer (arrows) in a dense breast seen on FFDM (Left) and DBT (Right).

Figure 5: FFDM (Left) and S-view Mammogram (Right) of the same breast; microcalcifications (arrows) are shown more clearly on the S-view that on the FFDM (note zoomed inserts).
References
Caumo, F. et al., 2017. Digital Breast Tomosynthesis with Synthesized Two-Dimensional Images versus Full-Field Digital Mammography for Population Screening: Outcomes from the Verona Screening Program. Radiology, 287(1).
Holt, J., Aujero, M., Gavenonis, S. & Benjamin, R., 2017. Clinical Performance of Synthesized Two-dimensional Mammography Combined with Tomosynthesis in a Large Screening Population. Radiology, p. published online.