
Imaging the Cervix – Part I
Pierre Vassallo
During pelvic ultrasound (US), the examiner consistently reports findings in the uterine body, endometrium and adnexa, while the cervix is often not mentioned. This probably results from a training in transabdominal pelvic US, since the cervix is poorly seen with this technique. On the other hand, endovaginal pelvic US with the excellent image quality obtainable on new devices, allows detailed assessment of the cervix.
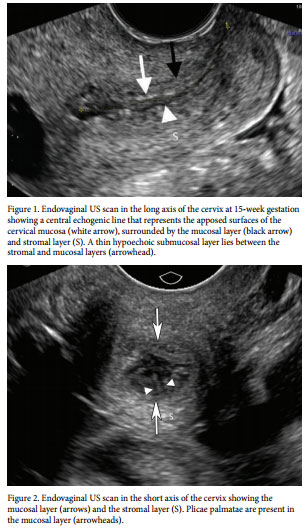
Endovaginal US can visualize the cervix in both the long axis and the short axis. The long axis lies parallel to the cervical canal, which extends from the internal os to the external os. In the long axis of the cervix, a central echogenic line is seen that correlates with the apposed surfaces of the anterior and posterior mucosal (or glandular) layers that line the cervical canal.
A small amount of fluid may be present within the cervical canal particularly in the periovulatory period. The mucosal layer, which lines the cervical canal, is iso- to hyperechoic and measures 2-4mm in thickness. Surrounding the mucosal layer is the stromal layer, which is moderately echogenic and forms the bulk of the cervix. Between the mucosal and stromal layer, a thin 1-2mm hypoechoic line may be seen that represents the submucosal layer (Figure 1).
Endovaginal US in the short axis shows the cervix as round or oval, containing a central echogenic spot representing the cervical canal surrounded by an iso- to hypoechoic mucosal layer, which is in turn surrounded by the echogenic stromal layer. Frequently, folds may be seen in the mucosal layer that represent the plicae palmatae (Figure 2).
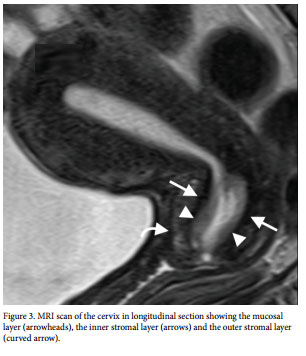
Magnetic resonance imaging (MRI) allows the best visualization of the cervix and is used to characterize indeterminate US abnormalities. MRI is the gold standard for staging cervical cancer. On T2-weighted images, the cervix shows a distinctive trilaminar appearance, with an innermost hyperintense layer measuring 3–8 mm that corresponds to mucosa and secretions, a middle low-signal-intensity layer representing the inner cervical stroma that measures 3–8 mm, and an outermost intermediate-signal-intensity layer representing the outer cervical stroma that measures 2–8 mm (Figure 3).
Congenital anomalies
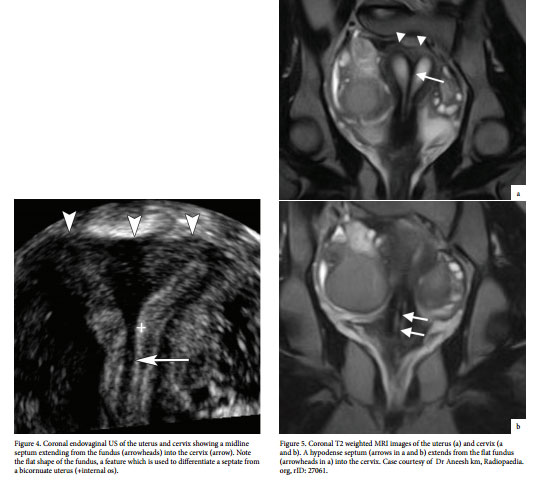
Congenital anomalies of the cervix are readily seen on US but are best demonstrated on MRI. One of the most common congenital anomalies is a septate uterus and cervix accounting for circa 45% of all congenital uterine anomalies. This results from incomplete fusion of the Müllerian ducts with persistence of an intervening septum. On US, it is best visualized in the coronal plane as a hypoechoic band extending from the uterine fundus into the cervix (Figure 4). The septum is composed mainly of fibrous stroma, which accounts for its hypoechogenicity. It shows increased vascularity on colour Doppler US in 70% of cases. MRI is the best imaging modality to evaluate a septate uterus and cervix; the fibrous septum is depicted as a low signal band extending from the flat uterine fundus into the cervix in the coronal plane (Figure 5). The septum may continue into the vagina in up to 25% of cases.
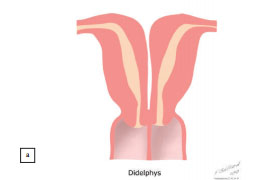
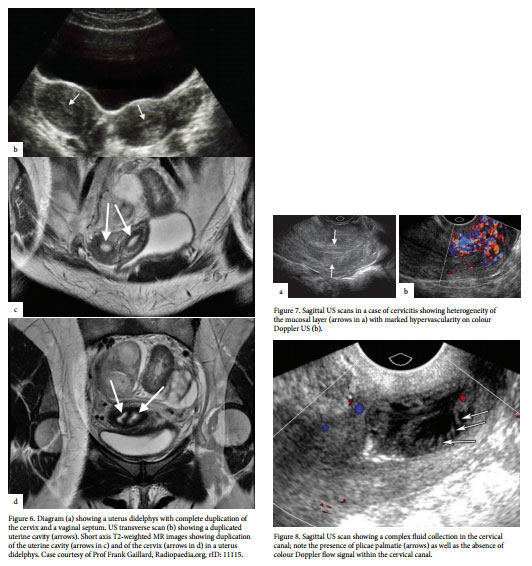
Uterus didelphys or “Double Uterus” represents a congenital anomaly where there is complete duplication of the endometrial cavity. The two endometrial cavities are separated not just by a fibrous septum as in a septate uterus but by a central stromal layer lined on either surface by mucosal layers. A uterus didelphys may contain two separate uterine cavities fusing into a single cervical canal or a fully duplicated cervix (Figure 6a). It may be difficult to distinguish a septate cervix from a duplicated cervix on ultrasound; in a duplicated cervix the band separating the two cervical canals is thicker that in a septate cervix (Figure 6b). Figures 6c and d illustrate separate endometrial cavities and cervical canals with a band of intervening stroma, clearly shown on MRI (Figure 6c and d).
Cervicitis
Cervicitis is the term used to describe cervical inflammation, which may be acute or chronic. This is most often caused by infection, although trauma, pelvic radiation, chemical irritation, and sometimes malignancy may also cause cervical inflammation. Microorganisms such as Trichomonas vaginalis, Candida albicans, herpes simplex virus (especially type 2), Neisseria gonorrhoeae and Chlamydia trachomatis can also cause cervicitis. Patients usually present with purulent cervical and vaginal discharge and may complain of pelvic discomfort. US findings of cervicitis can be subtle or even completely occult, especially if the condition is of a chronic nature or if the patient is examined during or after effective antimicrobial treatment. At US, the cervix in patients with acute cervicitis shows a diffusely heterogeneous echotexture of the cervical mucosa and stroma (Figure 7a), with markedly increased vascularity on Doppler US imaging (Figure 7b). Hypervascularity can also be seen in cervical carcinoma, however in cervicitis, no mass lesion is seen. Cervicitis may lead to cervical canal stenosis and complex fluid collections within the cervical canal. Such fluid collections may mimic a cystic tumour in the cervical canal on US, however colour Doppler evaluation would confirm the avascular nature of the endocervical content (Figure 8).
Benign Uterine Growths
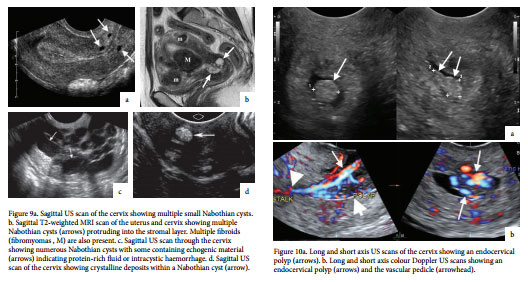
Nabothian cysts are one of the most common findings on pelvic ultrasound. Nabothian cysts are mucus-retention or epithelialinclusion cysts that arise from an obstruction of endocervical glands by proliferating squamous epithelium. They may or may not be associated with previous clinical or subclinical episodes of cervicitis. Nabothian cysts may appear as anechoic fluid collections in the mucosal layer of the cervical canal (Figure 9a), but can be quite large and protrude into the stromal layer (Figure 9b). They may also contain echogenic material due to secondary intracystic haemorrhage (Figure 9c) and even calcifications (Figure 9d).
Cervical polyps are the most common endocervical lesions and are also the most common cause for intermenstrual bleeding. They occur most commonly in women between the ages of 30 and 40 years of age and 25% are associated with an endometrial polyp. Cervical polyps appear slightly hyperechoic compared to the cervical mucosa on US (Figure 10a), they are seen to move on pressure with the endovaginal probe and are frequently noted to have a vascular pedicle on colour Doppler US (Figure 10b).
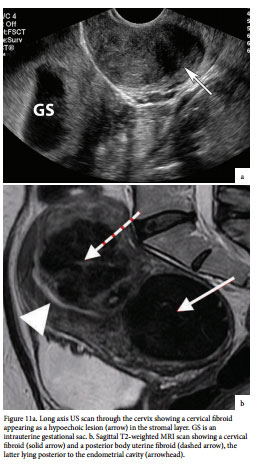
Cervical fibroids or fibromyomas are not uncommon and may lead to some diagnostic difficulty. They may also result in shoulder impaction during child birth. Cervical fibroids are seen as hypoechoic mass lesions in the cervical stroma (Figure 11a). MRI is the most reliable modality to confirm the diagnosis, which shows low signal on all imaging sequences (Figure 11b). The second part of this article will discuss imaging of endometriosis in the cervical canal and also cervical cancer. The importance of imaging in staging of cervical cancer will be presented.