Diagnostic Imaging of Mass Lesions in the Hand
Pierre Vassallo
M ass lesions in the hand are not common. However, a run of clinical cases that the author encountered in recent weeks prompted him to write on the subject. Lesions of the epidermis and dermis and those of bony origin will not be discussed in this article
Ganglion cyst
The most common soft tissue mass lesion found in the hand is a ganglion or ganglion cyst as it is sometimes referred to. These lesions originate from tendon sheaths or joint synovial lining following (usually repetitive) trauma. They are clinically hard and well-defined and are usually painful. They tend to move along with movement of the related tendons. Ultrasound is usually sufficient to confirm a ganglion as a fluid-filled welldefined lesion occasionally containing some debris related to a tendon or joint (Fig 1). These lesions frequently resolve spontaneously with rest or they may be ruptured by manual massage. Traditionally, they were smashed with a heavy book. The Bible served this purpose well; in fact ganglion cysts are also known as Bible cysts. Additional treatment options include ultrasound-guided steroid injection and surgical excision.
Lipomas
Lipomas were once believed to be rare in the hand, but are now considered common in this location. Most often they are found in subcutaneous layer, but they occasionally occur in deeper layers particularly intramuscularly. Clinically they present as a mass showing insidious growth. Most are solitary and asymptomatic and only come to clinical attention when they are of cosmetic concern or when they become large enough to create mechanical impairment. About 20% of hand lipomas present with pain and tenderness, and less commonly sensory deficit due to nerve impingement. Lipomas appear as welldefined echogenic masses on ultrasound that can be clearly distinguished from surrounding structures (Fig 2). Lipomas show high T1 and low T2 signal that is in contrast to most other solid lesions. Solid tumors are usually further investigated with MRI, which is very useful in identifying tissue type (Fig 3).
Subcutaneous haemangiomas
Subcutaneous haemangiomas consist primarily of a cluster of blood vessels within a solid soft tissue mass. The palm was the most common location in the clinical cases reviewed by the author. Progressive enlargement of the lesion and throbbing pain were the most common symptoms. Characteristic features of haemangiomas include compressibility, poorly defined margins, bluish discolouration of overlying skin, and enlargement of the lesion when the venous return is obstructed or the extremity elevated. Ultrasound shows a soft tissue mass with varying vascularity that may be seen as sparse channels on grey-scale ultrasound (Fig 4a) with possibly a feeding artery on colour Doppler ultrasound (Fig 4b). Haemangiomas are usually surgically excised with ligation of the feeding vessels as distant from the tumor as possible in order to diminish the chances of recurrence.
Nerve sheath tumors
Nerve sheath tumors may occur at any location in the body where nervous tissue is present. These tumors often affect the function of the nerve, causing pain and disability. A large majority of peripheral nerve tumors are benign and include neurofibromas or schwannomas. Some occur as part of a more generalized condition such as neurofibromatosis or schwannomatosis, both of which are genetic disorders of the nervous system. Malignant nerve sheath tumors are rare; they are more commonly seen in cases of neurofibromatosis type 1. Peripheral nerve sheath tumors are often hypoechoic and may show posterior acoustic enhancement. The presence of peripheral nerve continuity suggests the diagnosis of peripheral nerve sheath tumor (Fig 5). Sonography cannot reliably distinguish neurofibromas from schwannomas.
Giant cell tumors
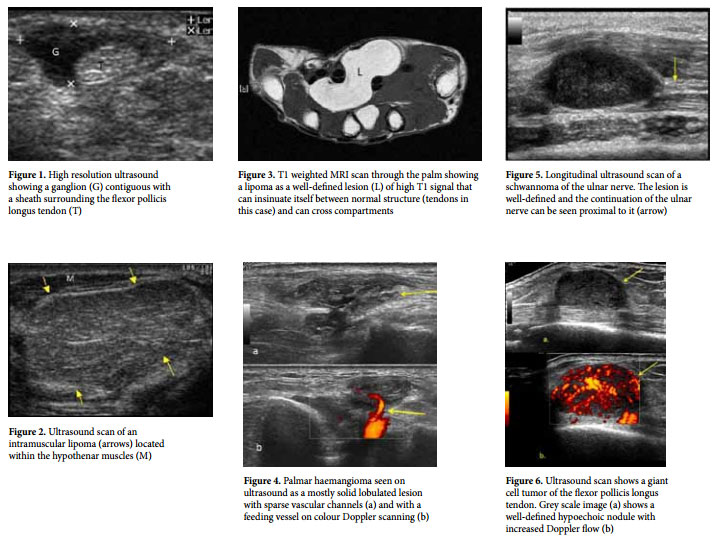
Giant cell tumors of the tendon sheath are benign tumors of unknown aetiology arising from the tendon sheath and are considered as a variant of pigmented villonodular synovitis. These lesions usually affect the volar aspect of the first three digits, much less commonly affecting the wrist. On ultrasound, the lesions are usually well-defined and hypoechoic and may be hypervascular on colour Doppler ultrasound (Fig 6). MRI scans show a usually well-defined lesion with low T1 and high T2 signal, demonstrating strong enhancement following intravenous contrast administration (Fig 7). These findings are characteristic of most tendon sheath lesions, and excision biopsy is the only means to obtain a histological diagnosis.
Fibromas
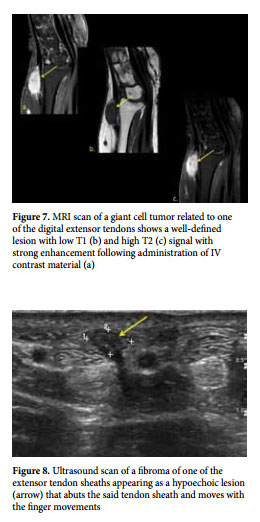
Fibromas of the flexor tendon sheath are rare benign tumours, which present as a firm, well-defined mass attached to the tendon sheath. Imaging findings are similar to those of giant cell tumors on both ultrasound and MRI, however fibromas tend to have a lower signal on T2 weighted images and show less enhancement with IV contrast material. On ultrasound they show as flat hypoechoic lesions that follow the tendon sheath and also tend to move with finger movements (Fig 8).
Dupuytren’s contracture
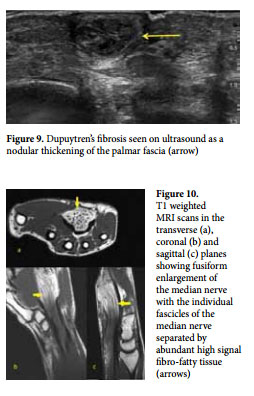
Dupuytren’s contracture is the proliferation of fibrous tissue within the palmar fascia of the hand, which causes subcutaneous nodules on the palmar surface of the distal crease of the hand. This normally progresses to the cords and bands and, finally, leads to the characteristic flexion contracture secondary to fibrous attachments to the underlying tendon sheath. Histologically and on imaging the appearance is similar to flexor sheath fibromas (Fig 9).
Fibrolipomatous hamartomas
Fibrolipomatous hamartomas are benign tumors usually affecting infants and less commonly children and young adults. The median nerve is the most commonly affected nerve (80% of cases) but other upper and lower limb nerves may be involved. The most common clinical presentation is that of a soft, slowly enlarging and often asymptomatic mass on the volar wrist frequently present since infancy. Occasionally, nerve compression will lead to symptoms of pain, paresthesia or carpal tunnel syndrome. It is postulated that this is a congenital abnormality of the growth of fibrofatty tissues that causes infiltration and fusiform nerve enlargement. Sonographic findings show hyperechoic tissue (echogenic fatty tissue) surrounding smooth round hypo- or anechoic fascicles. MRI is the preferred imaging modality and shows fusiform nerve enlargement with abundant fibro-fatty tissue surrounding individual nerve fascicles. Enlarged nerve bundles look like serpentine or tubular structures on all imaging modalities (Fig 10). The MRI appearance of fibrolipomatous hamartomas is pathognomonic.
The above article does not claim to cover all differential diagnostic possibilities of soft tissue masses of the hand. However it discusses the more common entities and their imaging features. High resolution ultrasound and MRI are the main imaging modalities that help not only to characterise the lesions, but also to evaluate their relationship to sensitive structures such as arteries and nerves. This information is useful in surgical planning. Some of the lesions have very similar imaging characteristics and biopsy is required in many cases to establish a diagnosis.