
COVID-19: A View from China
Dr Gauden Galea MD, MSc(Lond), FFPH
WHO Representative, China
The views expressed are those of the author alone and do not necessarily represent those of WHO.
March 1, 2019
It is Day 61 of the COVID-19 epidemic, counting from the date of closure of the Huanan Seafood Wholesale Market in Wuhan, Hubei Province, in China. In the two months since then, the country has reported 80,026 cumulatively diagnosed cases (202 new cases since Day 60) and 2,912 cumulative deaths (42 new deaths since Day 60). These figures include 32,652 current cases, 7,110 of which are severe cases. A WHO-China Joint Mission on COVID-19 has just released its report on 28 February. This article summarises key findings of that report for the attention of the Maltese medical community as it prepares for the possibility of Malta’s own outbreak.
China has demonstrated that it is possible to change the course of COVID-19 outbreaks
Figure 1. Epidemic curve by date of onset. China CDC: China Centers for Disease Control and Prevention; WHC: Wuhan Health Commission; NHC: National Health Commission; PHEIC: Public Health Emergency of International Concern; NCIP: Chinese name for the disease officially called COVID-19 by WHO.
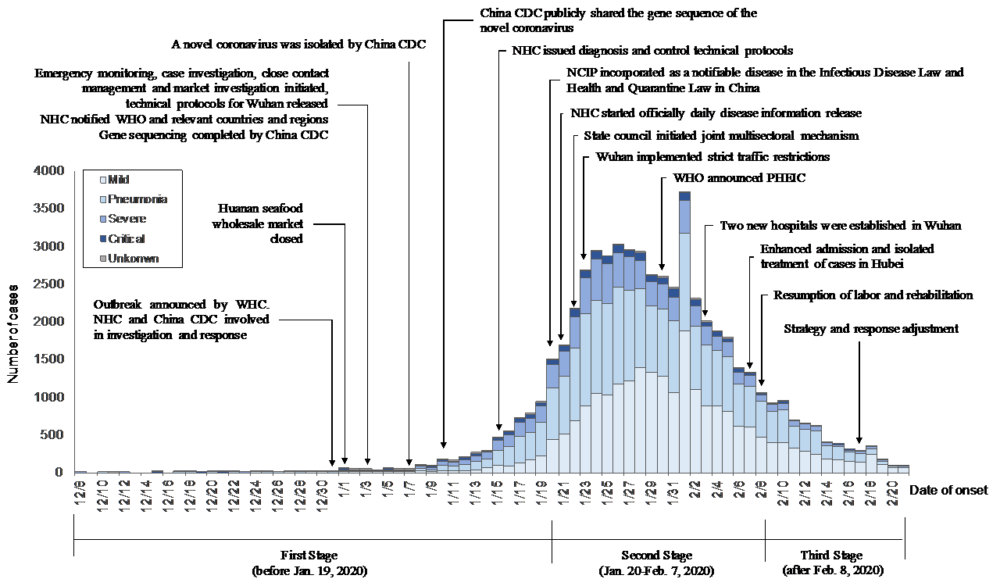
The epidemic curve (taken from the WHO-China Joint Mission Report) should be a much taller normal distribution based on the reproduction number ranging between 2.0-2.5 estimated from models of the transmission dynamics of the virus. Instead, the curve is blunted, flattened, skewed to the right, indicating that in the last week of January, some intervention changed the course, slowed down the spread, and initiated a plateau, then a decline. In the absence of a vaccine or therapy, China used time-honoured measures of containment and social distancing that have been part of the arsenal of public health for centuries. It is possible to emulate the success of China, but the measures call for collective action with great determination.
Five Steps to Containment
The containment of an outbreak of COVID-19 needs five steps of increasing intensity:
- The universal population measures of hand hygiene, food hygiene, respiratory etiquette, and social distancing came first in China and were aggressively promoted in social media and all traditional media. China also required mask wearing for all.
- Case isolation: The high transmissibility of the virus and the infective nature of even mild cases requires active and rigorous case finding and isolation. Case definitions should not unduly restrict eligibility for testing – within the limits of kit availability and lab capacity. Cases should be rapidly diagnosed and taken out of circulation; China initially took two weeks on average to identify a case; that has now been reduced to three days from onset.
- Close contact quarantine: Close contacts of all cases should similarly be rigorously quarantined for 14 days beyond the last exposure to the case. With each infected individual leading on average to two more cases among their close contacts, rigorously enforced quarantine is the only way to effectively break the chains.
- Suspension of public gatherings: China set the example during the Chinese New Year Festival (a two week period that started on 25th January this year). Temple fairs, cinemas, restaurants, and all large scale festivities were cancelled. Schools were closed (still closed at the time of writing). The traditional week of public holiday was extended.
- Movement restrictions: At its extreme, these involved the complete closure of Wuhan, a city of 11 million people. In other cities lesser measures were adopted but still quite effective in restricting movement on a large scale, including the closure of express ways into certain large cities.
These five steps were not applied evenly throughout China, but a tailored approach to applying these measures was taken in different provinces, based on the prevalence of infection. In a province where there are no cases, universal precautions and public mobilisation will be appropriate, but in one where there is sustained community transmission, the more powerful of these interventions (suspension of mass gatherings and movement restrictions) will be needed. In order to gauge the level of community transmission, testing should be applied liberally to samples from the Influenza-like Illness surveillance system (the ILI sentinel system) but also opportunistically on suspicious cases presenting in general practice or ambulatory settings.
Prepare for an outbreak
Even as these containment measures were proving successful, China still prepared and is preparing still for the possibility of larger numbers of cases. Lessons for Malta include:
- President Xi Jinping and Premier Li Keqiang took personal responsibility and leadership for the response. A Joint Prevention and Control Task Force repurposed to the whole machinery of government and all government departments were required to make the fight against the virus their top priority.
- Collective action by the population is essential. In China it is inspiring to see the thousands of health care workers and volunteers mobilised to the front line in Wuhan. It is also important to note the acceptance by the population and community grid system (a form of neighbourhood watch) to monitor and enforce quarantine. Clear guidelines are available: for landlords, for business owners, for hotel managers, and all the population, from taxi drivers to security guards are informed of their part in the battle.
- While the measures taken to contain the epidemic have been available since the Middle Ages, China’s approach to them has been highly technological. Big data has been deployed to track cell phones and to monitor quarantine. Artificial Intelligence has been deployed in the diagnosis of CT scans. Virtual hospitals and telemedicine have been used to reduce the number of routine visits that people have to make for other reasons to hospital.
- Given that severe and critical cases may take three to six weeks to recover or die, in a community outbreak there will be high demand for oxygen, for ventilation, and the occupancy of intensive care beds will be prolonged. The availability of life support (beds and ITU staff) for prolonged periods will be one of the determinants of case fatality.
- Throughout all this, access to health care expertise is essential, and the protection of health care workers through strengthened infection prevention and control procedures is essential. Indeed, evidence in China suggests that many of the HCWs infected acquired the virus earlier on, when possibly the use of personal protection and universal precautions may not have been as rigorous.
Further reading
- The Novel Coronavirus Pneumonia Emergency Response Epidemiology Team. The Epidemiological Characteristics of an Outbreak of 2019 Novel Coronavirus Diseases (COVID-19). China CDC Weekly, 2020, 2(8): 113-122. http://weekly.chinacdc.cn/en/article/id/e53946e2-c6c4-41e9-9a9b-fea8db1a8f51
- WHO-China Joint Mission on COVID-19. Report of the Joint Mission. WHO (Geneva). 2020. https://www.who.int/docs/default-source/coronaviruse/who-china-joint-mission-on-covid-19-final-report.pdf
- WHO Technical Guidance Website: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance