
US-Guided Treatment of Calcific Rotator Cuff Tendonopathy
Pierre Vassallo
Calcium hydroxyapatite crystal deposits in the rotator cuff are a common source of shoulder pain. Calcified tendinitis can lead to chronic disability and may interfere with daily living activities. Traditionally, the initial conservative therapeutic approach consists of oral nonsteroidal anti-inflammatory drugs, physical rehabilitation to prevent loss of joint mobility and local steroid injections. When conservative treatment fails, open surgical or arthroscopic excision of calcium deposits can be performed.
Removal of the calcium deposits from the tendon significantly accelerates healing of the tendonopathy, however, the open surgical and even arthroscopic techniques are prone to prolonged post-operative disability and complications such as reflex sympathetic muscle dystrophy. Image-guided interventions to remove calcium deposits in the rotator cuff have been used as far back as 30 years ago. However, these procedures were mainly done under X-ray fluoroscopic guidance and utilized two large-bore needles, one to inject normal saline and the other to fragment the calcification and aspirate the fluid containing the calcium fragments. Use of these needles generally resulted in significant damage to the tendon.
More recently, ultrasound (US) (figure 1) has been utilized to guide the intervention; this allows better visualization of smaller deposits, while avoiding radiation exposure to the patient and the performer. In addition, a single small-bore needle technique is being used to minimize the extent of trauma to tendon. Combining US-guidance with the use of a small-bore single needle reduces collateral damage.
The procedure requires a full initial US assessment of the rotator cuff to establish calcification size, location, and number as well as the presence of local tendon swelling, rotator cuff tears, cortical irregularities of the greater tuberosity and the presence of fluid in the subacromio-subdeltoid bursa. This information should be documented prior to the intervention. Calcification of the rotator cuff is depicted as a hyperechoic focus with or without acoustic shadowing, or occasionally, only by a faint shadow (figure 2).
For calcifications in the supraspinatus and infraspinatus tendons, the procedure is best performed with the patient in the seated position preferably on a swivel chair. For calcifications in the subscapularis tendon, the supine position is used.
The procedure is performed by using sterile technique and surgical gloves. A skin mark is placed on the skin for localization of the calcified deposit. Then the skin is cleaned and antiseptically draped. The transducer head is also antiseptically cleaned. Local anesthesia (1% lidocaine hydrochloride) is administered in the subdeltoid bursa adjacent to the tendon. After identifying and localizing the calcified deposit at US, the calcification is punctured under constant US monitoring using a 22 to 25-gauge needle. A horizontal course and an antero-posterior direction of the needle are favored because of easier US localization of the needle and calcification; in addition, having the syringe in the horizontal position results in sedimentation of any aspirated calcium fragments to the dependent portion of the syringe, while keeping the syringe nozzle free, minimizing the risk of blockage.
Once positioned in the center of a calcification, the tip of the needle is gently rotated followed by an attempt to aspirate the fragmented calcified material by using a 5–10mL syringe filled with lidocaine 1% (figure 3). Occasionally, fragmentation of the calcified deposit is performed better by initially injecting lidocaine into the calcification followed by aspiration. The success of aspiration varies depending on the calcification consistency at the time of the procedure. When the calcification is very hard and no material can be extracted, grinding of the calcified deposit is performed by using gentle rotation of the needle tip; this has the added advantage of accelerating any spontaneous resorption. When the calcification has a paste-like consistency, a lavage manoeuver is possible by using the lidocaine-containing syringe without any attached tubing. Successive propulsion and aspiration with the syringe plunger is performed to retrieve the calcified material, with constant US monitoring of the needle position.
The extracted calcium is readily identified in the syringe as a white cloud-like substance mixing with the lidocaine that would then deposit in the dependent portion of the syringe (figure 4); this is why retaining the syringe in a horizontal position prevents the risk of injecting calcium back into the rotator cuff and also prevents nozzle and needle blockage.
Following this maneuver, the needle tip is retrieved slightly and 40mg Depo-Medrone® (methylprednisolone acetate) combined with 1–2mlL of bupivacaine 0.5% or with 1–2mL of lidocaine 1% are injected at the surface of the calcified tendon in the subacromial-subdeltoid bursa. Patients are thereafter discharged with a prescription for oral nonsteroidal anti-inflammatory agents for the eventuality of exacerbation of pain in the shoulder during the day following the procedure. Complications following the above procedure are virtually non-existent.
Patients should be re-evaluated after an 8-10 week period. At this stage, correlation with the pre-therapeutic US findings is crucial in order to assess the impact of the intervention. Aspiration of calcium deposits from the rotator cuff is not always completely successful. The amount of calcium that is removed is proportional to the extent of clinical improvement seen on follow-up evaluation. Partial evacuation of calcium deposits however, results in a decrease in pressure within the inflammatory area in the tendon, which accelerates healing. Depending on different study groups, this technique has a success rate of 60-75% with a significant reduction in morbidity as compared to an open surgical or arthroscopic procedure.
Figure Legends
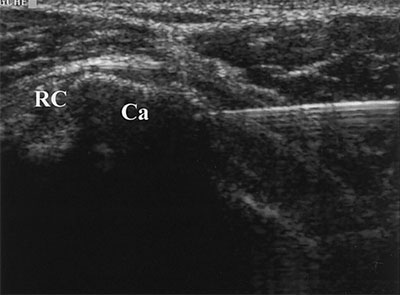
Figure 1. Longitudinal US scans of a normal rotator cuff (RC) of right shoulder. C = cartilage of the humeral head, D = deltoid muscle, H = humeral head.
Figure 2. Longitudinal US scans of a calcium (Ca) deposit in the supraspinatus tendon of the left shoulder (rotator cuff: RC) with hyperechoic superior contour and posterior acoustic shadow (solid arrows). H = humeral head.
Figure 3. Transverse scans of US-guided percutaneous needle aspiration in the left shoulder. RC = rotator cuff. Scan shows the needle as it enters the calcification (Ca). The distal part of the needle is not visible because of the posterior acoustic shadow generated by the calcium.
Figure 4. Syringe after rotator cuff calcification lavage with lidocaine. White calcified material (∗) has accumulated at the bottom.