Urography – changing strategies
Pierre Vassallo
U rography is defined as the imaging of the urinary tract, so essentially any form of imaging done for the urinary system falls under this heading. There are two main reasons for imaging the urinary tract: renal colic and haematuria (particularly painless haematuria).
The first imaging studies to directly target the urinary tract were plain X-rays, which could detect the presence of a stone along the urinary tract and possibly just identify the renal outline. However, <80% of stones are visible on plain X-rays even with today’s digital technology, whilst a renal mass would need to be at the edge of the kidney and be large enough to deform the renal outline in order to be detected on plain X-rays. The presence of gas and stool in the colon often obscures the urinary tract on plain X-rays severely limiting its value.
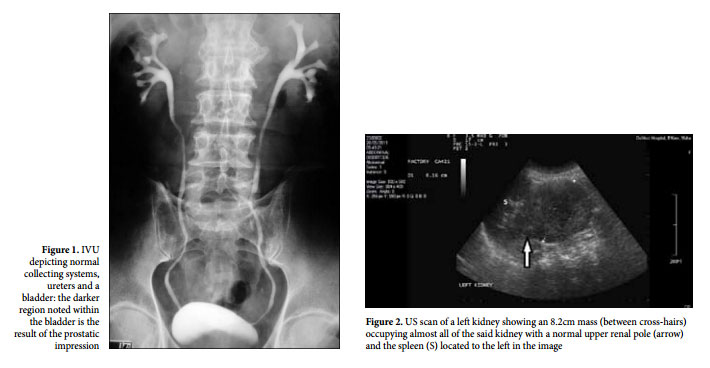
X-ray based intravenous urography (IVU) was later developed (Figure 1), which for several decades was the primary imaging modality for the urinary tract. This technique was first described in 1923, when Rowntree and co-workers injected 10% sodium iodide intravenously and noted that it enhanced the renal parenchyma. Sodium iodide is excreted through the urinary tract and this was visible on X-ray imaging. This was later combined with conventional tomography in an attempt to visualise the renal parenchyma in more detail and to detect small filling defects in the collecting system. However, even with the inclusion of conventional tomograms, IVU was virtually useless for imaging renal masses (MRI) to help reach a diagnosis.
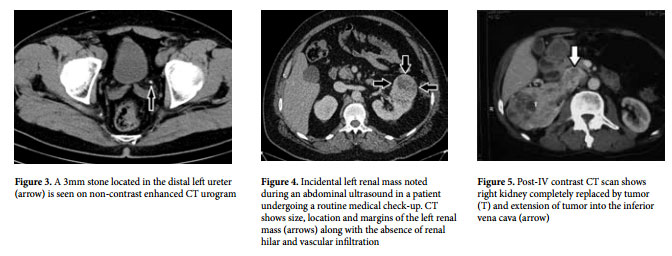
US is an excellent tool for evaluating the urinary system and improving technologies have come to provide detailed morphological depiction of kidneys and bladder (Figure 2). However, due to their retroperitoneal location, the ureters are not visible on ultrasound. Until recently, US did not provide any information on renal function, but with the recent introduction of contrast-enhanced US, this is likely to change. Notwithstanding the fact that US is an excellent first imaging modality when investigating painless haematuria, in case of painful haematuria or suspicion of renal colic, a CT urogram is more appropriate as the first imaging exam.
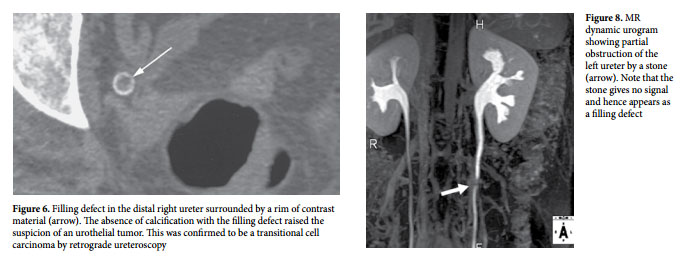
CT urography is the cross-sectional equivalent of the X-ray IVU, but has the major advantage of having a much higher soft tissue resolution and has no interference from gas and stool within the bowel. CT detects urinary tract stones with much greater accuracy that any other technique, including MRI, with detection rates reaching 100% even for stones as small as 1mm in diameter (Figure 3). The only known exceptions are stones related to treatment with antiretroviral agents used in the treatment of AIDS; these medications have a tendency to crystallize within the urinary tract and are non-radiopaque making them invisible on CT. The presence of such stones may be diagnosed through knowledge of the clinical history and indirectly through the presence of obstruction caused by the stone. No intravenous contrast material is required to detect stones on CT urography, which is particularly advantageous in those patients with impaired renal function.
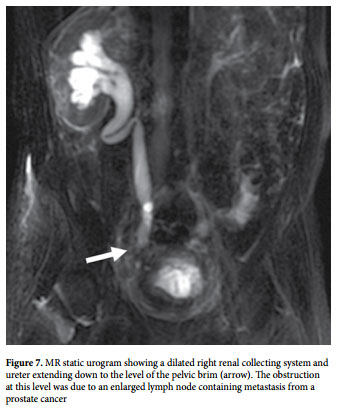
Intravenous contrast injection is required in cases of painless haematuria and in those individuals with either abnormal findings on the non-contrast scan or where there is clinical suspicion of a renal mass. The contrast-enhanced ??????????? changing strategies urogrAphy pierre vassallo 29 CT urogram shows the exact size of the renal mass (Figure 4), whether there is extension of the lesion through Gerota’s fascia or there is the presence or otherwise of hilar and intravascular extension (Figure 5). All these criteria help characterise the lesion, but more importantly assist with surgical planning. This information is required to decide whether either a partial or a total nephrectomy should be performed. Other important information that is visualised by CT urography is the presence of a synchronous lesion in the opposite kidney, as well as lymph node or distant (e.g. liver, lung or bone) metastasis. Delayed imaging after intravenous contrast material injection results in filling of the collecting systems and ureter as well as the bladder. Small urothelial tumors are best seen in these delayed scans (Figure 6).
MR urography is a more recent imaging modality that has potential benefits but also has its limitations. MR urography is insensitive to calculi. Examinations times are longer, spatial image resolution is lower that CT or IVU, it is more susceptible to motion artefacts and it is more expensive that other urographic modalities. However, it utilises no ionising radiation and is therefore more suitable for the paediatric population and during pregnancy. Tissue contrast resolution is also higher in MR urography than in CT urography or US, making it more useful in patients with impaired renal function in whom intravenous contrast material administration is not indicated. The MR urography protocol is divided into two parts: (a) the static fluid imaging part, in which heavily T2 (water)-weighted images are obtained to depict the collecting system, ureters and bladder in both 2D and 3D modes, and (b) the dynamic contrast enhanced imaging part, which uses T1 (fat)-weighted images and intravenous contrast material injection similar to the early phases of an IVU but depicts cross-sectional anatomy and can therefore more accurately display pathology.
Static-fluid MR urography obtains images of the free fluid within the ureters and if serial images are obtained and played in a cine loop, temporary ureteric narrowing due to peristalsis can be distinguished from fixed stenosis that may be caused by inflammatory disease or a neoplasm. Static-fluid MR urography is best suited to imaging dilated collecting systems and ureters as occurs in the presence of obstruction (Figure 7). It is particularly useful to evaluate paediatric patients with congenital causes of urinary tract obstruction and in ureteric obstruction occurring during pregnancy.