Ultrasound of the wrist ligaments
Pierre Vassallo
Injuries of the intrinsic and extrinsic wrist ligaments can lead to chronic wrist pain and carpal instability, while injuries of the triangular fibrocartilage complex (TFCC) are a frequent cause of ulnar-sided wrist pain. In the recent past, magnetic resonance (MR) arthrography was the preferred imaging modality for the evaluation of these structures, but good results can also achieved with standard MR imaging, computed tomographic (CT) arthrography and more recently ultrasonography (US). Advantages of US of the wrist over MR imaging and MR arthrography include: lower cost, no intraarticular injection of contrast material, no ionizing radiation, no limitations due to MR incompatible implants, and real-time visualisation with possible dynamic evaluation. However US is operator dependent and requires high quality equipment. Imaging should start with radiography, which helps provide crucial information on the osseous anatomy and is an important adjunct in the initial clinical assessment of these structures in everyday orthopedic practice. US has proved valuable in the evaluation of the wrist and hand. It allows visualization of foreign bodies, various tendon injuries and abnormalities, retinacula, ganglion cysts, annular pulleys, vessels, and nerves, including evaluation of carpal tunnel syndrome, joint effusions, and inflammatory arthropathies. The use of US in the evaluation of the wrist ligaments and TFCC is still evolving and has shown promising results.
The anatomy of the ligaments of the wrist is complex. The ligaments are divided into the intrinsic group, which includes those ligaments that lie in between and bridge the carpal bones, and the extrinsic group, which refers to those ligaments lie on the surface of the carpal bones and that attach the palmar or dorsal surfaces of the carpal bones to each other and to the radius or ulna. This arrangement may be oversimplified by stating that the intrinsic ligaments are intraarticular while the extrinsic ones are extra-articular.
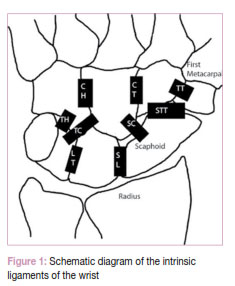
The intrinsic ligaments bridge the carpal bones and are named by the bones that attach to. These include the scapho-lunate, luno-triquetral, trapeziotrapezoid, trapezo-capitate, capitohamate, scapho-trapezio-trapezoid, scapho-capitate and triquetro-capitate ligaments (Figure 1). Of these ligaments, the two most frequently injured are the scapho-lunate ligament (SLL) and the luno-triquetral ligament (LTL). Both the palmar and dorsal components of these ligaments are visible on US (Figures 2-5).
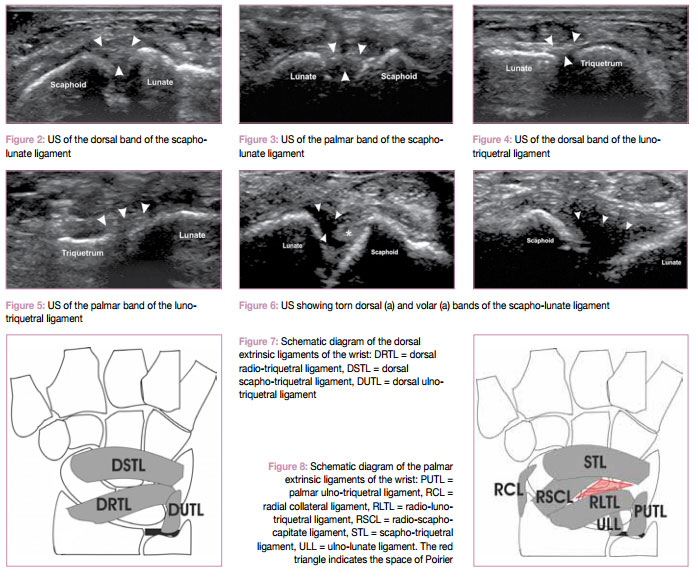
Disruption of the SLL and LTL may cause pain and instability. On plain radiographs, an intercarpal distance of 4mm or more taken with a clenched fist is indicative of an intrinsic ligament tear. A distance less than 4 but greater than 2mm is equivocal, while a distance less than 2mm is normal. It is well known that intrinsic intercarpal ligamentous disruption occurs due to age degeneration and is usually asymptomatic. Ultrasound is able to visualise tears of both the dorsal and volar bands of the SLL (Figure 6a and b) and LTL ligaments.
The extrinsic ligaments are divided into two groups, those on the dorsal aspect and those on the palmar aspect (Figures 7 and 8). At the palmar aspect of the wrist, a triangular area of weakness (called the space of Poirier) is present that lies between the proximal and distal rows of ligaments. This accounts for the frequency in perilunate and lunate injuries and dislocations. The extrinsic ligaments are stiffer, while the intrinsic ligaments are more elastic and allow a greater degree of intercarpal motion.
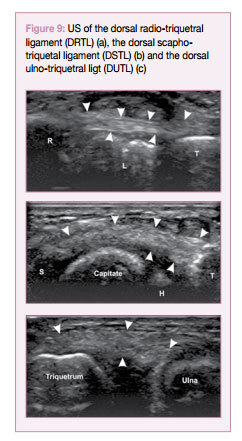
Ultrasound can visualised all dorsal and palmar extrinsic ligaments with great accuracy (Figures 9 and 10) and tears of these ligaments can be efficiently confirmed with this technique.
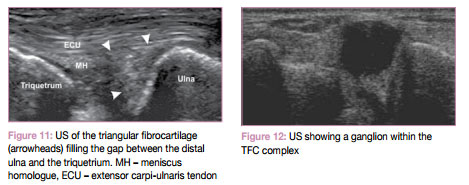
The triangular fibrocartilage complex (TFC) is also well visualised (Figure 11). Various types of injury/degeneration of the TFC complex are readily confirmed by ultrasound (Figures 12 and 13).
In conclusion, US shows promising results in the evaluation of the varying normal and abnormal anatomy of the intrinsic and extrinsic wrist ligaments and the TFCC, and provides an alternative imaging method to MR imaging, MR arthrography, and CT arthrography in the evaluation of these structures. With the constant improvement in US technology, standardisation of imaging techniques, increased operator experience, dynamic imaging, and clinical correlation, US may is playing an increasing role in the evaluation of the intrinsic and the extrinsic wrist ligaments and the TFCC.