Ultrasound-Guided Thyroid Fine Needle Aspiration
Pierre Vassallo
U ltrasound (US)-guided FNA lends itself particularly well to lesions in superficial organs such as the thyroid, lymph nodes and the breast. However, since it is less traumatic than core biopsy, it is safer for use in highly vascular organs such as the thyroid gland. Smaller nodules are more amnable to FNA, while larger nodules are better sampled with core biopsy.
Focal thyroid lesions
The Society of Radiologists in Ultrasound suggests that FNA should be considered for a thyroid nodule 1.0cm or more at the largest diameter if microcalcifications are present and for a nodule 1.5cm or larger if the nodule is solid or if there are coarse calcifications within the nodule
In cases of multiple thyroid nodules, the risk of an individual nodule being cancerous is decreased but the prevalence of thyroid cancer does not differ between patients with a solitary nodule and those with multiple nodules. Recent literature indicates that patients with multiple thyroid nodules have the same risk Ultrasound-Guided Thyroid Fine Needle Aspiration Pierre Vassallo of developing thyroid malignancy as patients with solitary thyroid nodules. Therefore in the presence of multiple nodules, FNA is indicated. However a meticulous search for suspicious ultrasound features should be made in order to identify the more suspicious nodules as sampling of all nodules is frequently not practical.
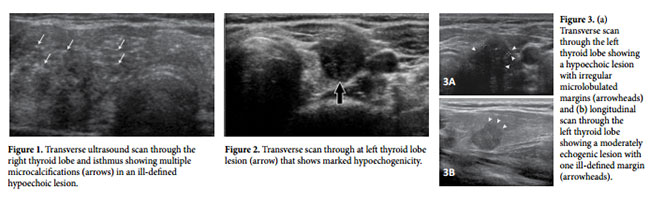
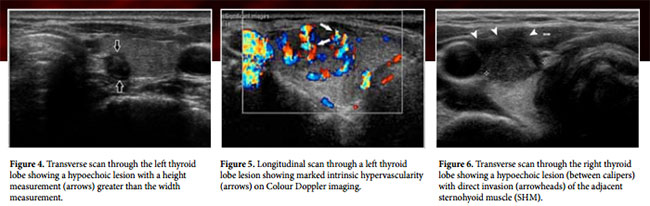
US features that are suggestive of malignancy include microcalcifications (Fig 1), marked hypoechogenicity (Fig 2), an irregular or microlobulated margin (Fig 3), a longitudinal dimension larger than the transverse dimension (Fig 4), high intrinsic vascularity (Fig 5), direct tumor invasion of adjacent soft tissue (Fig 6), and metastasis to one or more lymph nodes (fig 7).
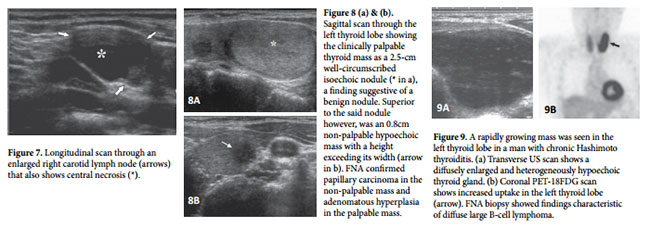
In cases with multiple thyroid nodules, US characteristics are more useful than nodule size for identifying nodules that are likely to be malignant. If only the dominant or largest nodule is aspirated, a thyroid cancer may be missed (Fig 8 a, b). Diagnostic US therefore should be performed to characterize all thyroid nodules prior to considering which one(s) to biopsy.
Diffuse Thyroid
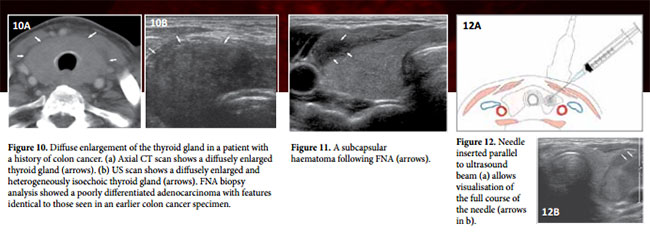
Lesions Among patients with autoimmune diseases such as Hashimoto thyroiditis, the rate of thyroid malignancy is similar to that among patients with a non-symptomatic thyroid gland. In cases in which Hashimoto thyroiditis manifests as a nodular lesion mimicking a thyroid neoplasm, FNA must be performed to rule out lymphoma and papillary carcinoma, either of which may coexist with Hashimoto thyroiditis (Fig 9 a, b). FNA is also required in cases of diffuse rapid enlargement of the thyroid gland, especially in patients older than 50 years, to rule out anaplastic carcinoma, metastasis, and lymphoma (Fig 10 a, b).
High Risk of Thyroid Cancer
The threshold for biopsy of a thyroid nodule in a patient with one or more risk factors for thyroid cancer is lower than that for biopsy in a patient without such risk factors. Risk factors for thyroid cancer include a family history of thyroid cancer, a history of head and neck irradiation, male gender, age of less than 30 years or more than 60 years, and a previous diagnosis of type 2 multiple endocrine neoplasia.
Procedure for performing an US-guided Thyroid FNA
Prior to performing thyroid FNA, the reasons for performing the procedure should be explained to the patient. These are (1) to reach a diagnosis and (2) possibly avoid surgery. The procedure for performing a thyroid FNA must be explained and informed consent obtained from the patient.
One should ask about known coagulation disorders and whether the patient is taking anticoagulation treatment; if no history of coagulation disorder or anticoagulation medication exists, it is not necessary to perform coagulation studies prior to FNA. If core biopsy is contemplated, coagulation studies are best performed prior to the biopsy.
Significant complications are rare. Most frequent (but also rare) complications are subcapsular haematomas (Fig 11). Even rarer is extensive extracapsular bleeding into the neck. Both complications are treated conservatively.
At the start of the procedure, the patient is placed in the supine position with a pillow under the shoulders to improve neck extension. The skin is cleansed with chlorhexidine solution, which is also used as the US medium (replacing US gel). Local anaesthetic is administered to skin and subcuteneous tissues with 1-2mL 1% lidocaine hydrochloride solution.
Initial scanning in the horizontal plane is performed to locate the lesion and evaluation with Colour Doppler Ultrasound identifies the location of large blood vessels that need to be avoided to minimize the likelihood of blood contamination of the specimen. The patient is instructed not to swallow or speak while the needle is in the thyroid gland
The probe is placed in the transverse plane with the needle/ syringe parallel to the plane of the probe with a medio-lateral or latero-medial approach (Fig 12a). Having the needle parallel to the plane of the beam improves visualisation of the needle tip (Fig 12b).
A 24-gauge needle is inserted into the solid portion of the nodule under US visualisation and when the needle tip is in position, it is moved vigorously in and out while being rotated to dislodge as much tissue as possible from the nodule into the needle bore. This is ideally performed until a small amount of tissue is seen in the hub of the needle. Aspiration may or may not be performed during the to-and-fro movement, but is best avoided in very vascular lesions as it is likely to cause specimen contamination with blood.
During the procedure, the needle tip should be placed into different parts of the nodule avoiding blood vessels; this will improve sample quality and reduces the sample inadequacy rate. Aspiration should not be performed while the needle is withdrawn. The procedure may be repeated especially if the sample obtained appears bloody.
After the procedure, adhesive plaster is applied, and the patient should be instructed to manually compress the skin entry site for a minimum of 30 minutes. The patient should be instructed to contact hospital staff or visit the emergency room if neck swelling occurs on the way home or at home.
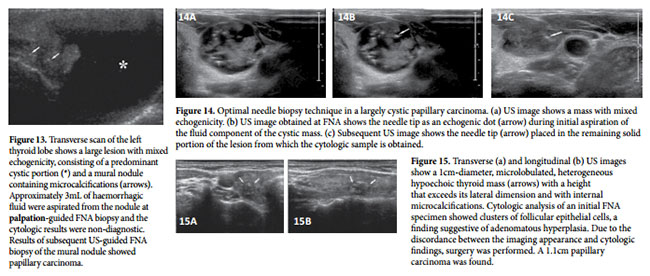
If a lesion contains both cystic and solid components, the solid component should be sampled (Fig 13). If the lesion contains a large fluid component, this is best to aspirate the fluid first and then perform a FNA on the remaining solid component (Fig 14).
A repeat FNA biopsy should be considered if there is discordance between the findings at imaging and those at cytologic analysis (Fig 15), a growing mass, a recurrent cyst, or an inadequate FNA sample. At least 3 months should be allowed to elapse after the initial FNA biopsy. The 3-month time lag before repeat FNA is recommended to avoid problems in cytologic interpretation that may be posed by reparative cellular atypia (e.g. marked nuclear chromatin clearing, grooves, or inclusions that may be mistaken for evidence of papillary carcinoma).
For follow-up of thyroid nodules with an initial benign cytologic diagnosis and without clinical or radiologic findings suggestive of malignancy, imaging surveillance is recommended rather than repeat US-guided FNA biopsy. If nodule size is stable, the interval before the next follow-up clinical examination or US evaluation may be prolonged.
Conclusion
US-guided FNA is useful for the diagnosis of palpable or non-palpable thyroid nodules. The routine use of this biopsy procedure has caused profound changes in the management of thyroid nodules. FNA biopsy allows prompt identification and treatment of thyroid malignancies and avoidance of unnecessary surgery in patients with benign lesions, thereby improving the overall quality of life for patients with thyroid nodules. Furthermore, FNA helps guide treatment and helps reduce the cost of care.
The adequacy of cytologic specimens depends on several factors, including the nodule characteristics and the FNA technique used. As the person performing FNA gains experience and as lesion targeting and localization with US become more accurate, the rate of sample inadequacy should decrease
To optimize the usefulness of FNA, every centre should strive to attain and maintain a high level of expertise in all aspects of aspiration and interpretation and, toward that end, should establish clinical guidelines tailored to its patient population and FNA biopsy results.