
The Value of Troponin assays in modern medical practice
Karl Cutajar
Cardiac troponins – C, I and T – form part of the troponin complex which is involved in the regulation of the calcium-mediated interaction of actin and myosin in myocytes.
Introduction
Biochemical and Physiological aspects
Cardiac troponins – C, I and T – form part of the troponin complex which is involved in the regulation of the calcium-mediated interaction of actin and myosin in myocytes.1 Each troponin has a different role in the above mentioned complex. Troponin C is involved in binding calcium, troponin I inhibits interaction of actin to myosin, while Troponin T binds to tropomyosin and facilitates muscle contraction.1
 |
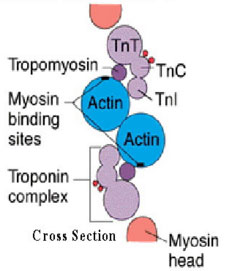 |
Figure 1. Schematic representation of the thin filament of the muscle myofibrils. Myosin is the principal protein from which the thick filaments are composed
Source: Tanindi A, Cemri M. Troponin elevation in conditions other than acute coronary syndromes. Vascular Health and Risk management 2011;7:597-603
Both skeletal as well as cardiac muscle types express troponin C, however the amino acid sequences of troponin I and troponin T are unique to cardiac muscle. It is the specificity of these latter troponins to cardiac muscle that allowed for the development of quantitative assays that detect elevations of troponins in the serum once released by damaged cardiac muscle tissue.1
The majority of Troponin I and C form part of the contractile apparatus of the muscle myofibril. A small fraction of the troponins is however free in the cytoplasm. This fact explains the relatively biphasic rise in serum troponin. The initial rise corresponds to the release of free cytoplasmic troponin. This is subsequently followed by a second rise – that corresponds to the dispersion of the myofibril-bound troponin complexes.1
Keeping the above mechanisms in mind, one notes that any form of damage to cardiac muscle may result in the release of the above proteins into the bloodstream. As acute coronary syndromes are the commonest cause of myocardial damage, the detection of elevated levels of troponin levels in the serum are often attributed to such events.2
Troponin: The ideal Cardiac biomarker
The earliest cardiac biomarkers used to detect myocardial ischemia included aspartate aminotransferase and lactate dehydrogenase isoenzymes, however these biomarkers were found to be poorly specific in view of the fact that they have a wide tissue ditribution.1 Eventually, creatine kinase (CK)-MB isoenzyme assays were posited as the gold standard investigations in the diagnosis of acute coronary syndromes (ACS).
CK-MB, whilst more specific for cardiac muscle, still constitutes around 1-3% of the CK found in skeletal muscle. It is also present in a small fraction in other organs such as the prostate, uterus and small bowel. Therefore in the setting of major injury to any of the above organs the specificity of CK in detecting myocardial damage is reduced.1
- CK-MB has gradually been sidestepped by cardiac troponin assays, which have ever since their initial use for the diagnosis of ACS, become more and more sensitive. 3 Nowadays the cardiac troponin testing is the preferred diagnostic test for ACS particularly for non-ST segment-elevation myocardial infarction (NSTEMI). The results from cardiac troponin testing guide the decision for the adequate intervention in patients in whom the diagnosis of ACS is not obvious from the clinical presentation and the findings on ECG.3
- Troponin I and T, when compared to other biomarkers, have both the highest sensitivity and specificity for cardiac ischemia.1 Between 1995 and 2007, the limit of detection of cardiac troponins fell from 0.5ng/mL to 0.006ng/mL, accounting for approximately a hundred-fold improvement in analytic sensitivity.3
However, whilst the increasing sensivity of troponin assays are allowing us to recognise and treat ACS earlier, the ever increasing sensitivity of these biomarkers is in itself inevitably associated with a reduction in the specificity of the test.3
The value of troponins in the diagnosis of ACS
Acute myocardial infarction (MI) is defined as necrosis of myocardial tissue. The diagnosis nowadays requires that there must be a rise or fall in troponin levels with at least one value above the 99th percentile of the upper reference limit of the normal healthy population as defined by European Society of Cardiology in 2007.1 In addition, there should be at least one of the following:
1. ECG changes indicative of ischemia (e.g. new ST/T wave changes or new LBBB)
2. Symptoms suggestive of ischemia, e.g. chest pain, diaphoresis, nausea, SOB or loss of consciousness
3. Imaging studies showing evidence of new wall motion abnormalities/loss of viable myocardium.1
In the past, the major limitation of cardiac troponins in aiding diagnosis of ACS was the fact that in the first few hours after an MI, plasma troponin levels would still be undetectable – secondary to the delayed increase in circulating levels of cardiac troponins. Generally the diagnosis would depend on monitoring the patient and taking serial blood samples over a 6-12 hour period.2 Nowadays with the high sensitivity troponin assays which are becoming available, it is recommended that the second specimen can be collected at 2-3 hours from the first specimen taken at presentation.3 This is a huge improvement as the longer the wait before a diagnosis is made (and any applicable intervention) the greater the morbidity and mortality. However, as mentioned earlier, the greater sensitivity of the troponin assays means that the number of patients with detectable Troponin elevations in the emergency department or other in-hospital settings, will increase as a result. This poses greater challenges on physicians to make a differential diagnosis. Non-ischemic causes of troponin elevation should thus always be kept in mind. One should always refer to the clinical picture, ECG and other available investigations.2
Non-ACS causes of elevated Troponins
Many cardiovascular and non-cardiovascular states are associated with elevated troponin levels. Atrial fibrillation, supraventricular tachycardias, heart failure, myocarditis and cardiac contusion are among the non-ACS causes of increased troponin levels.
Increased toponins levels are also noted to be present in conditions such as Chronic obstructive pulmonary disease (COPD) and acute pulmonary embolism. These conditions cause right heart strain which in turn might explain the link with the elevated troponin levels. End-stage renal disease (ESRD) is also commonly associated with an elevated troponin level. In fact, it is thought that if all the patients with ESRD were to have their troponin levels measured, in over 50% of the patients they would be elevated. This is often attributed to the impaired excretion of troponin, however it might also be the result of small areas of clinically silent myocardial necrosis.2
Intracranial pathology is another non-cardiac cause of elevated troponin levels. Not uncommonly, patients with intracranial hemorrhages (e.g. subarachnoid haemorrhages) and acute strokes are found to have elevated troponin levels. Furthermore these individuals may also have electrocardiographic changes, such as cardiac rythm disurbances, which may further confuse the picture. One theory for the above is that myocardial ischemia develops pursuant to any pre-existing cardiac tachycardia/hypertension. Howwver, nowadays the most widely accepted explanation is the “cathecolamine hypothesis”. It is believed that acute brain injury causes a massive release of cathecolamines (norepinephrine) from sympathetic nerve terminals innervating the myocardium. This subsequently leads to myocyte necrosis and contractile dysfunction resulting in the ECG changes and troponin release into the plasma.2
Non-thrombotic causes of elevated troponin levels11. Direct myocardial damage
• Cardiac contusions
• Direct current cardioversion
• Cardiac infiltrative disorders
• Chemotherapy
• Myocarditis
• Cardiac transplantation (immune-mediated reactions)
2. Myocardial strain
• COPD
• CHF
• Acute pulmonary embolism
3. Chronic renal insufficiency
4. Intracranial pathology (subarachnoid haemorrhages/acute stroke)
5. Demand ischemia (in absence of ACS)
• Left ventricular hypertrophy
• Anaemia
• Hypotension
• Hypovolaemia
• Atrial Fibrillation/Supraventricular tachycardia
The Prognostic role of Cardiac Troponins
Apart from their diagnostic role, cardiac troponins also yield prognostic information. Patients having clinical evidence of ischemia and high levels of troponin in the circulation tend to have a worse prognosis. Studies have shown that peak troponin T levels in the circulation actually correlate well with the infarct size. The greater the extent of the troponin rise, the poorer the prognosis.1
Conclusion
Early detection of MI is crucial in ensuring better outcomes. Troponin assays are essential in establishing an earlier diagnosis. However, the ever-increasing sensitivity of these assays is associated with a decrease in their specificity. One should consider the clinical picture as well as other available investigations, and always take at least two serial troponin readings.
References
1. Daubert MA, Jeremias A. The utility of troponin measurement to detect myocardial infarction: review of the current findings. Vascular Health and Risk management 2010:6;691-9.
2. Tanindi A, Cemri M. Troponin elevation in conditions other than acute coronary syndromes. Vascular Health and Risk management 2011:7;597-603.
3. Mahajan V, Jarolim P. How to Interpret Elevated Cardiac Troponin Levels. Circulation 2011:124;2350-4.