
The Cholesterol Controversy – The Series
Albert Cilia Vincenti
Atherosclerosis remains the number one cause of morbidity and mortality in most countries. After almost a century of research, the creation of a huge industry in blood cholesterol testing and marketing of statins, as well as significant advances in interventional cardiology and coronary by-pass surgery, the causation and pathogenesis of atherosclerosis remains, as yet, not only poorly understood, but actually controversial.
If the risk factors for atherosclerosis remain poorly understood, and some very controversial, it is no wonder that in spite of improved survival from coronary heart disease (CHD) (due to all the efforts and funds spent on investigations and treatment), there is no good evidence that the incidence of atherosclerosis has significantly decreased.
Many doctors leave medical school with a poor knowledge of physiology and biochemistry and come to rely blindly on information imparted from pharmaceutical companies, the latter also influencing clinical research with their funding. So let’s go back to some basic science and clinical research from as far back as the 1960s which, although apparently largely forgotten, remains valid.
Blood insulin (hyperinsulinaemia and insulin resistance) has been claimed to be the most important predictor of CHD.1-12 However, this has been largely ignored because the “dietary saturated fat, blood cholesterol and CHD” theory has prevailed and spawned the multi-billion statin industry, directed at lowering LDL-cholesterol. But around 50% of patients hospitalised with CHD are reported to have total and LDL-cholesterol levels within normal limits.13
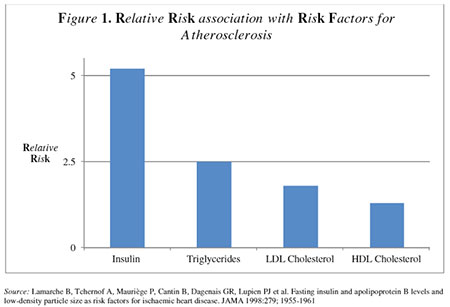
A study which looked at fasting blood insulin levels compared with conventional risk factors, to see which was more predictive of developing CHD over a 5-year period in clinically disease-free individuals, found that fasting insulin levels were more than twice as predictive compared to LDL-cholesterol (Figure 1).14 Triglycerides (TRG) were also more predictive than LDL15,16 In fact, one of the first signs of hyperinsulinaemia is increased TRG. Although HDL by itself is a less powerful predictor than LDL, when the increase in risk of elevated TRG is multiplied by the increase in risk of decreased HDL, the result is very close to fasting insulin as risk predictor for CHD. The fasting TRG/HDL ratio is in fact a surrogate marker for fasting insulin.17-20
You will remember from previous instalments that what routine laboratories measure as LDL consists of two fractions, one large and light and the other small and dense. The latter is very prone to oxidation and claimed to be related to atherosclerosis.21 The other fraction is reckoned not be related to CHD. In routine laboratory estimates of LDL levels one does not know which LDL fraction predominates. However, high fasting TRG/HDL ratios have been associated with high levels of the small dense LDL fraction, and the TRG/HDL ratio is therefore a convenient surrogate marker for the small dense LDL fraction.22
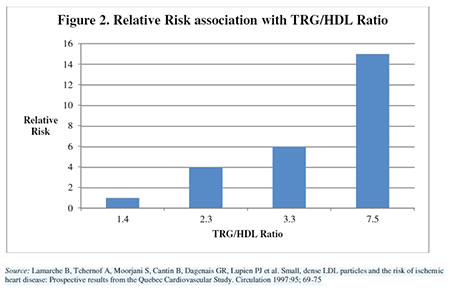
A study comparing patients who had survived their first heart attack with matched patients without a history of CHD, found (Figure 2) that those with the highest TRG/HDL ratios were 16 times more likely to have a heart attack than those with lower ratios.23 This is a dramatic finding. Do you know which drug lowers the TRG/HDL ratio? No, it’s not statins. It’s a low-carbohydrate with adequate protein and saturated and monounsaturated fat diet.24,25
The conventional wisdom driving the “dietary saturated fat, blood cholesterol and CHD” band-wagon continues to advise doctors and the general public to reduce dietary fat at all costs. But dietary fat has no direct effect on blood insulin. Even way back in 1997, leading nutritional researchers wrote in the New England Journal of Medicine that there is no persuasive data supporting the hypothesis that a low-fat, high-carbohydrate diet has any long-term benefit in treating obesity, CHD and cancer.26 Why? Because each of these diseases is associated with hyperinsulinaemia. Fat has no effect on insulin secretion, whereas carbohydrates have a major stimulatory effect.
In conclusion, it is most unfortunate that the US governmental nutritional advice continues to recommend severe restriction of dietary saturated fat. Also worrying are, (a) the continuing conventional wisdom that LDL is the prime indicator of CHD risk, (b) the lack of recognition that the TRG/HDL ratio is the most predictive of all the routine blood lipid profiles, and (c) that statin therapy protocols based mainly on routine LDL levels (without knowledge of LDL dense sub-fractions) are of suspect validity. Statins might be a blunderbuss therapy whose positive effect on established CHD may be only via their anti-inflammatory action, similar to the far cheaper aspirin.
Whether adding more expensive predictive tests, such as high-sensitivity C-reactive protein (HsCRP) and the PLACtest®, improves mortality from CHD (compared to the routine TRG/HDL ratio), is not yet clearly established.
References
- Bao W et al. Persistent elevation of plasma insulin levels is associated with increased cardiovascular risk in children and young adults. Circulation, 1996: 93; 54-59.
- Black HR. The coronary disease paradox. The role of hyperinsulinemia and insulin resistance and implications for therapy. J Cardiovascular Pharmacol, 1990: 15; 26S-38S.
- Depres JP et al. Hyperinsulinemia as an independent risk factor for ischemic heart disease. New Engl J Med, 1996: 334; 952-957.
- Duimetiere PE et al. Relationship of plasma insulin to the incidence of myocardial infarction and coronary heart disease mortality in a middle-aged population. Diabetologia, 1980: 19; 205-210.
- Fontbonne A. Why can high insulin levels indicate a risk for coronary artery disease? Diabetologia, 1994:37; 953-955.
- Job FP et al. Hyperinsulinism in patients with coronary artery disease. Coronary Artery Disease, 1994: 5; 487-494.
- Reaven GM & Hoffman B. The role of insulin resistance and hyperinsulinemia in coronary artery disease. Metab, 1992: 41; 16-19.
- Stern MP &Haffner SM. Body fat distribution and hyperinsulinemia as risk factors for diabetes and cardiovascular disease. Atherosclerosis, 1986: 6; 123-130.
- Stout R. The relationship of abnormal circulating insulin levels to atherosclerosis. Atherosclerosis, 1977: 27; 1-13.
- Stout R. Insulin and atheroma – an update. Lancet, 1987: I; 1077-1079.
- Zavaroni I et al. Risk factors for coronary artery disease in healthy persons with hyperinsulinemia and normal blood glucose tolerance. N Engl J Med, 1989: 320; 702-706.
- Perry IJ et al. Serum insulin and incident coronary heart disease in middle-aged British men. Am J Epidemiol, 1996: 144; 224-234.
- 13. RidkerPM et al. High-sensitivity C-reactive protein, inflammation and cardiovascular risk: from concept to clinical practice to clinical benefit. American Heart Journal, 2004: 148; 819-826.
- Lamarche B et al. Fasting insulin and apolipoprotein B levels and low-density particle size as risk factors for ischaemic heart disease. JAMA, 1998: 279; 1955-19 61.
- Austin MA. Plasma triglyceride and coronary artery disease. Arterioscler Thromb Vasc Biol, 1991: 11; 2-14.
- Davignon J & Cohn JS. Triglycerides: a risk factor for coronary heart disease. Atherosclerosis, 1996: 124; S57-S64.
- Karhapaa P et al. Isolated low HDL cholesterol: An insulin resistant state. Diabetes, 1994: 43; 411-417.
- Lamarche B et al. Triglycerides and HDL-cholesterol as risk factors for ischemic heart disease: Results from the Quebec Cardiovascular Study. Atherosclerosis, 1996: 119; 235-245.
- Laws A et al. Relation of fasting insulin concentration to high density lipoprotein cholesterol and triglyceride concentration in men. Arterioscler Thromb, 1991: 11, 1636-1642.
- Laws A &Reaven GM. Evidence for an independent relationship between insulin resistance and fasting HDL-cholesterol, triglyceride and insulin concentration. J Int Med, 1992: 231; 25-30.
- Tchernof A et al. The dense LDL phenotype: Association with plasma lipoprotein levels, visceral obesity and hyperinsulinaemia in men. Diabetes Care, 1996: 19; 629-637.
- McNamaraJR et al. Change in LDL particle size is associated with change in plasma triglyceride concentration. Arteriosler Thromb Vasc Biol, 1992: 12; 1284-1290.
- Lamarche B et al. Small, dense LDL particles and the risk of ischemic heart disease: Prospective results from the Quebec Cardiovascular Study. Circulation, 1997: 95; 69-75.
- Parks EJ &Hellerstein MK. Carbohydrate-induced hypertriacylglycerolemia: historical perspective and review of biological mechanisms. Am J Clin Nutr, 2000: 71; 412-433.
- Campbell LV et al. The high-monounsaturated fat diet as a practical alternative for non-insulin dependent diabetes mellitus. Diabetes Care, 1994: 17; 177-182.
- Katan MB et al. Beyond low-fat diets. N Engl J Med, 1997: 337; 563-566.