
Piles and more … dealing with incompetent veins
by Adrian Micallef
The day that man took his first steps on his two hind legs is considered a milestone in the evolutionary dominance of mankind. Yet this feat has borne with it one huge burden – the human being is just about the only species to suffer from varicose veins and haemorrhoids, the visible effects of venous insufficiency.
Chronic venous disease (CVD) has been described as ‘an abnormally functioning venous system caused by venous valvular incompetence with or without associated venous outflow obstruction, which may affect the superficial venous system, the deep venous system, or both’.[1] With the minor inclusion of post-thrombotic syndrome, the majority of CVD can be attributed to chronic venous insufficiency (CVI) which is the pathophysiological mechanism for both abnormal leg veins and haemorrhoids.
Leg veins
The primary pathology here is incompetence of the supporting valves within the deep and superficial venous systems as well as the perforating veins connecting these two systems,[2],[3] leading to backflow and clinical sequelae. Valve defects may have a genetic component, and a family history of CVD is a strong risk factor for developing features of this condition. However, external factors definitely play a part in the onset and severity of the clinical expression. A sedentary lifestyle, prolonged standing and wearing of high heels all interfere with the calf muscle pump which is indispensible for efficient venous return. Obesity and pregnancy interfere with venous return and increase back pressure. There is also hormonal influence, which contributes to the increased prevalence of venous problems in women especially in multiparae and those on hormone treatment. Hot environments, cardiac insufficiency and, of course, age are other risk factors for developing CVI.

Figure 1: Initial signs of chronic venous insufficiency
Clinical features vary with the severity of CVI: in general, the more proximal the valve failure, the more severe the effects. Symptoms include leg heaviness or pain and night-time cramps, worsened with heat and immobility and improving with activity and elevation. The signs of CVI start initially with the appearance of superficial terminal tributaries such as telangiectasis and reticular veins progressing through to varicose veins, oedema, varicose eczema and pigmentation, and ultimately to the appearance of ulceration.
Haemorrhoids
Haemmorhoids can be considered as the local (anal) expression of CVI, with varicosities of the rectal venous plexus being initially asymptomatic but eventually progressing to discomfort, itching, bleeding and eventually acute inflammation and thrombosis. Apart from the general lifestyle risk factors described for leg veins, additional local risks factors include change in bowel habits, prolonged coughing or sneezing, rectal pathology and local trauma (including intercourse).
Management of CVI
The therapeutic objectives of treating CVI in leg veins and haemorrhoids are threefold: (1) immediate clinical improvement; (2) prevention of evolution of venous disease; and (3) prevention of complications such as post-thrombotic syndrome. Unsightly spider and reticular veins are often a reason for referral for cosmetic removal although they may be symptomatic, and can be treated with procedures like sclerotherapy[4] and laser ablation. Sclerotherapy[5] and endovenous ablation with laser or radiofrequency[6] are also effective minimally invasive treatments for minor varicosities, but for advanced disease surgery, vein ligation or stripping is often necessary. Haemorrhoids may also be managed conservatively initially with topical treatment but eventually require interventions such as sclerotherapy, excision or rubber band ligation.
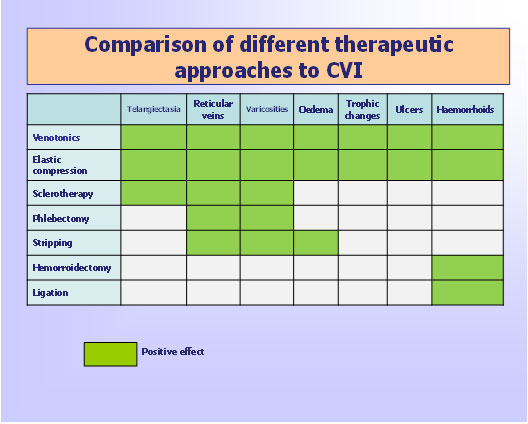
Figure 2: Comparison of different therapeutic approaches to chronic venous insufficiency
Phlebotonics (venotonics) are a class of recently developed compounds, mostly plant-derived, which have been clinically proven to have a corrective effect on CVI by improving venous tone, decreasing capillary permeability, increasing lymphatic drainage, and reducing release of inflammatory mediators by inhibiting migration and activation of leucocytes.[7] Diosmin is a well studied venotonic in both leg vein insufficiency[8] and haemorrhoids;[9] it is a natural flavonoid and comes in either micronized or coaggregated (600mg) forms; the latter allows for a more convenient dosage regimen for the conditions indicated. This is due to the coaggregation of diosmin, which increases residence time of the active principle in the organism, because of its entry in the enterohepatic cycle.
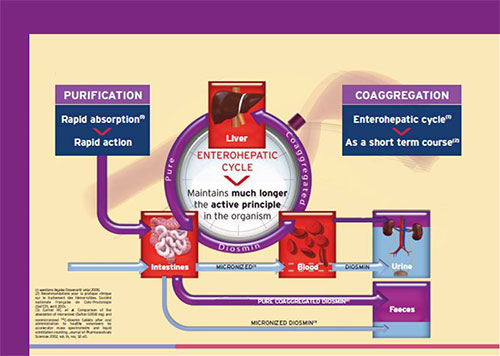
Figure 3: Differences in the absorptive pathways of micronized and coaggregated disomin
Of course, improving general lifestyle measures are central to the long-term success of these interventions. Weight loss, a more active lifestyle, wearing correct footwear (maximum of 3-4cm heels), a high-fibre diet, avoidance of hot environment, as well as wearing of support garments and avoiding constrictive clothing are all factors which should be highlighted in the family doctor’s surgery when managing this medically important condition.
References
[1] Porter JM: reporting standards in venous disease. J. Vasc. Surg. 1995, 21: 635 – 645.
[2] Laurence D, Fish PJ, Kakkar VV. Blood flow in incompetent perforating veins. Lancet 1997; 1: 117 – 118.
[3] Mullin GM, Scott HG, Smith PDC, Sarr JH. A reassessment of the role of perforating veins in chronic venous insufficiency. Phlebology 1990; 5: 85 – 94.
[4] Biegeleisen HI. Varicose veins, related diseases and sclerotherapy: a guide for practitioners. Montreal, Canada. Eden Press, 1984.
[5] Peribok E. Injection therapy of varicose veins: a method of obliterating varicosities with small doses of sclerosing agent. Angiology 1974; 25: 393 – 405.
[6] Rautio T, Ohinmaa A, Perala J, et al. Endovenous obliteration versus conventional stripping operation in the treatment of primary varicose veins: a randomized controlled trial with comparison of costs. J. Vasc. Surg. 2002, 35: 958 – 965.
[7] Perrin M, Geroulakos G. Pharmacological treatment of chronic venous disorders. Phlebology 2007; 14 (1): 23 – 30.
[8] Carpentier P, Mathieu M, Ceranic M. Evaluation of clinical efficacy of a venotonic drug: lessons of a therapeutic trial with hemisynthesis diosmin in ‘heavy legs syndrome’. J. Mal. Vasc. 1998, 23 (2): 106 – 112.
[9] Kecmanovic D, Pavlov M, Ceranic M et al. The use of Phlebodia in the management of bleeding non-prolapsed haemorrhoids. Acta. Chir. Jugosl. 2005, 14: 115 – 116.