
Pancreatic Cancer
by Pierre Vassallo MD PhD FACA Artz fur Radiologie
Consultant Radiologist
Pancreatic cancer is the fourth leading cause of death from cancer in the developed world. It has a dismal prognosis, with a mortality rate similar to its incidence. The overall 5-year survival rate is less than 5%. Early diagnosis and resection remain the only potential cure, but only a minority(5–30%) of tumors are detected when they are still resectable. However screening has not proved to be effective in the general population and is not recommended.
Spiral Computed Tomography (CT) is the best technique currently available for detecting and staging pancreatic cancer. MRI is useful for equivocal cases and allows better visualisation of the common bile duct through MRCP (MR Cholangio-pancreatography), which may be helpful in operative planning. Ultrasound is often the first exam to detect a pancreatic cancer in those patients presenting with jaundice, but more accurate staging with Spiral CT is required to plan treatment.
SpiralCT technology has seen major advances over the past 15 years with progress from single slice to multislice techniques and ultrashort rotation times, with the result that large areas of anatomy can be imaged with exquisite detail in a relatively short breath hold. Power injectors are now utilized to administer timed bolus injections of contrast material, which allow imaging at different phases (arterial, venous and delayed) of organ perfusion. Carefully timed scan acquisitionmaximizes the difference in enhancement between the neoplasmand the pancreatic parenchyma and allows accurate local anddistant staging. In addition, angiographic display of the local venous and arterial anatomy and TNM staging data (not usually used in radiographic reporting) are provided by spiral CT, which are crucial to surgical planning and are importantfor deciding on optimal therapy and neoadjuvant therapy.
During the late arterial phase of perfusion, the normal pancreas shows marked enhancement (figure 1), and imaging during this phase maximizes attenuationdifferences between the hypovascular tumor and the surroundinghypervascular normal parenchyma (figure 2). Usually, the tumor can be clearly seen againstthe enhanced background pancreatic parenchyma. Secondarysigns of malignancy such as pancreatic ductal or biliary dilatationor vascular occlusion can also be used to aid in tumor localization. About 10% of pancreatic adenocarcinomas have the same attenuation as background pancreatic parenchyma, making diagnosis more difficult. In such cases these secondary signs can be extremelyuseful (figure 3). The ’double duct sign’, best seen on ultrasound (figure 4), is a reliable indicator of an obstructinglesion, although it is not specific for pancreatic adenocarcinoma; this is caused by obstruction of the distal pancreatic and common bile ducts, which are therefore seen as two adjacent dilated ducts.
Staging of pancreatic cancer follows the TNM classification (Table 1). Resectibility is staged according to size of the tumor and presence of nodal or extranodal metastases (Table 2). Most patientsin whom resection appears to be viable at radiologic assessmentwill undergo laparoscopy prior to surgical exploration to ruleout small peritoneal implants or liver disease, the presenceof which precludes curative resection.
Approximately 90% of pancreatic adenocarcinomas manifest asa focal mass, with the remainder manifesting as more diffuseinvolvement. Radiologic imaging is highly sensitive for assessmentof the T stage. T1 and T2 tumors are distinguished on the basisof size, and this assessment can usually be accurately made on the basis of spiral CT imaging (figure 5). T3 disease is defined as extension into the peripancreatic soft tissues,without invasion into the celiac axis or superior mesenteric artery (SMA) (figure 6),which invasion characterizes a T4 tumor (figure 7). Lymph node (figure 8) and extranodal (figures 9 & 10) metastases are well assessed by spiral CT.
Spiral CT is well suited for both tumordetection and assessment of resectability, but recently, endoscopic US also appears to be playing a complementary role in tumor assessment and lymph node staging, sinceit allows sampling of any suspect lymph nodes that are present.Comparative studies suggest that when preoperative staging isperformed with both multidetector CT and endoscopic US, withone of the modalities being used for initial screening and theother in potentially resectable cases, the two modalities playcomplementary roles.
|
Table 1: TNM Classification |
|
| Tumor Staging | |
| Tx | Tumor not assessed |
| Tis | Carcinoma in-situ |
| T1 | Tumor < or = 2cm in diameter and confined to the pancreas |
| T2 | Tumor >2cm in diameter and confined to the pancreas |
| T3 | Tumor extends outside pancreas but does not involve celiac axis or SMA |
| T4 | Tumor involves celiac axis or SMA |
| Lymph node Staging | |
| Nx | Lymph nodes not assessed |
| N0 | Regional nodes not involved |
| N1 | Regional nodes involved |
| Metastases (extranodal) | |
| Mx | Metastases not assessed |
| M0 | No metastases |
| M1 | Metastases present eg liver, lung, peritoneum |
|
Table 2: Resectibility according to TNM stage |
||
| Stage 1 | Resectible | T1 or T2, N0, M0 |
| Stage 2 | Usually Resectible | T1 or T2, N1, M0 T3, N0 or N1, M0 |
| Stage 3 | Unresectible | T4, N0 or N1, M0 |
| Stage 4 | Unresectible | T any, N any, M1 |
Figure Legends
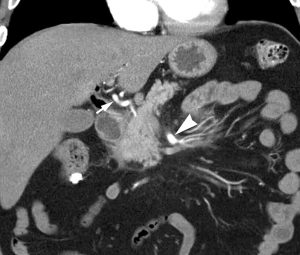
Figure 1. Coronal reformatted pancreatic parenchymal phase image shows intense enhancement of the normal pancreas. Note the excellent enhancement of the common hepatic artery (arrow) and the superior mesenteric artery (SMA) (arrowhead).

Figure 2. Contrast-enhanced CT scan shows a large, locally unresectable adenocarcinoma of the pancreatic head (arrow). Note the difference in attenuation between the tumor and the avidly enhancing normal pancreas.
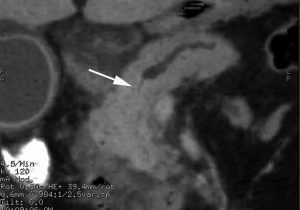
Figure 3. Abrupt cut-off of the pancreatic duct (arrow) in the region of the neck of the pancreas. No mass was visualized in the pancreas at CT.
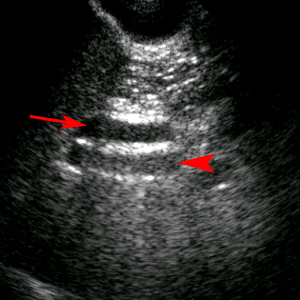
Figure 4. Double duct sign seen on ultrasound with a dilated common bile duct (arrow) lying anterior to the portal vein (arrowhead).

Figure 5. Coronal reformatted pancreatic parenchymal phase image shows a focal hypoattenuating tumor (arrow). Whipple resection confirmed a T2 tumor.
Figure 6. Large exophytic mass (arrows) arising from the neck of the pancreas and invading the stomach (arrowhead), a finding that represents a radiologic T3 tumor.
Figure 7. Infiltration of mesenteric root (arrows) with encased branches of the enhancing SMA.
Figure 8. CT scan shows a large pancreatic adenocarcinoma (arrowhead) as well as multiple surrounding peripancreatic lymph nodes (arrows).
Figure 9. Contrast-enhanced portal venous phase CT scan demonstrates a metastatic lesion in the liver (arrow).

Figure 10. Contrast-enhanced portal venous phase image shows a nodule on the inner surface of the peritoneum (arrow), consistent with peritoneal metastases. Arrowhead indicates the primary (pancreatic) tumor.