
Omeprazole-induced Delirium
Mark Abela, Nicola Aquilina, Alex Attard
Introduction
Delirium is a common manifestation in the elderly, with studies quoting a prevalence of up to 14% in the community in those aged 85 years and older.1 It occurs in 10-34% of patients living in long term care facilities,2 and occurs in 30% of patients presenting to the accident and emergency departments.3 Despite the fact that 10-42% suffer from delirium during a hospital stay, complicating 17-61% of major surgical procedures, it is unfortunately only recognized in 20-50% of cases.1,4 Despite the higher prevalence in the elderly population, it may present in all age groups, identified as per the ‘American Psychiatric Association’ (APA) Diagnostic and Statistical Manual (DSM-IV-TR and DSM-V Proposed Revision) criteria (Table 1).5
| 1. Altered consciousness with inattention difficulties
2. Cognitive or perceptual disturbances (unrelated to dementia) 3. Acute onset of symptoms (hours to days), typically fluctuating in nature 4. History, clinical assessment and investigations suggestive of organic causes for symptoms (including medication) |
Table 1. Diagnostic and statistical manual criteria (DSM-IV-TR and DSM-V).5
Medications are potential causes for delirium, accounting for as much as 39% of cases of delirium in the elderly, with the latter population being more at risk than other age groups due to altered pharmacokinetic and pharmacodynamics associated with the aging process.6
Proton pump inhibitors (PPIs) in particular are known to cause neuropsychiatric symptoms. One such PPI is omeprazole, a racemic mixture of two active enantiomers, classified as an inhibitor of the H+/K+-ATPase found on gastric parietal cells.7 Omeprazole-induced delirium has been documented in literature. One study on a small subgroup of cancer patients documented that histamine receptor 2 antagonists, also used as a treatment for gastritis, were more commonly associated with delirium than PPIs.8 That said, such cases have all been associated with metabolic and electrolyte disturbances, most notably hyponatremia and hypomagnesemia.7,9 We would like to report a case of omeprazole-induced delirium which clearly correlates with the time of its administration and omission. To our knowledge, this is the first case to document such a causal relationship without any other causes of delirium such a PPI-induced electrolyte disturbances.
Case Report
An eighty-five year old gentleman was admitted under surgical care because of a possible upper gastrointestinal (GI) bleed. He was previously well, with no relevant past medical history and fully independent prior to admission. On initial assessment at the emergency department, he was alert and oriented, haemodynamically stable and neurologically intact. In view of his severe epigastric pain, he was started on 40mg twice a day of intravenous omeprazole (Losec®), a proton-pump inhibitor, as part of the standard management protocol, which was later given as tablets. Twelve hours later, the patient appeared to be acutely confused, delirious and uncooperative. These symptoms got progressively worse during his admission. A collateral history from his relatives did not reveal any remarkable evidence of erratic alcohol or other drug dependence. Physical examination was unremarkable.
The patient was inattentive and incoherent, and thinking was clearly disorganised, with an altered level of consciousness manifesting itself as hyperactivity, reported by various nursing personnel. These symptoms were acute in onset and fluctuating. The acute fluctuating cognitive disturbance with the impression that the cause of the symptoms was organic in origin supported the diagnosis of delirium as per the Assessment Method (CAM) and APA DSM-IV-TR and DSM-V diagnostic criteria.5,6
Investigation of his epigastric pain did not reveal evidence of any acute GI bleeding and a diagnosis of probable gastritis was made. However, the persistence of delirium beyond the initial few days of admission prompted further investigations (Table 2)5 in order to identify any possible contributing factor towards the delirium, including electrolyte disturbances, metabolic disorders, sepsis, hypoxia, constipation, organ failure, and hypoxia, amongst others.10
Blood Tests
· Complete blood count
· Electrolytes (sodium, potassium, chloride, calcium, magnesium, phosphate, iron profile)
· Liver function tests including bilirubin, albumin, liver enzymes, ammonia
· Endocrine investigations including thyroid function tests, folate, vitamin B12
· Blood glucose
· Blood cultures
· Arterial Blood Gases (for Hypoxia and Hypercapnia)
· Toxicology
· Inflammatory markers including Estimated Sedimentaiton Rate (ESR), C-reactive protein (CRP), ferritin.
Urine Tests
· Urinalysis
· Urine Cultures
Neuroimaging
· CT Brain
· Electroencephalography
Others
· CSF Analysis (Biochemistry and Cytology)
· ECG
· Pulse Oximetry
· Chest X-Ray
· Abdominal X-Ray
Table 2. Basic investigations for diagnosing cause for delirium.5
Brain computer tomography (CT) scan and Electroencephalogram (EEG) are most often recommended to exclude acute (which need immediate management) or chronic intracranial pathologies such as a cerebrovascular event or a newly diagnosed space-occupying lesion. Despite them being used to identify or confirm specific diagnoses, thereby allowing a clinician to manage the patient accordingly, one should keep in mind that both CT and EEG have very high false negative (17%) and false positive (22%) rates. One should therefore understand that further tests such as magnetic resonance imaging (MRI) may be needed if there is a diagnostic suspicion, even if results are initially normal. That said, one would expect a higher diagnostic yield with CT in patients with focal neurological deficits.11 The CT scan revealed only an element of brain atrophy, which was thought to be consistent with this patients’ age. There was no evidence of acute infarction or any brain pathology. The background EEG showed a generalised slowing of the background rhythm with no focal or epileptiform features, consistent with a non-specific encephalopathy (Figure 1).
This patient was not started on any medication, other than omeprazole during his hospital stay, and therefore the possibility of a drug-induced delirium was not considered immediately. However, as a last attempt, the omeprazole was stopped and he was given ranitidine instead for his GI symptoms. Twelve hours later, the patient was back to his pre-morbid state, fully oriented, talkative, independent and co-operative with doctors and paramedical staff. After an 8 day hospital stay, he was discharged.
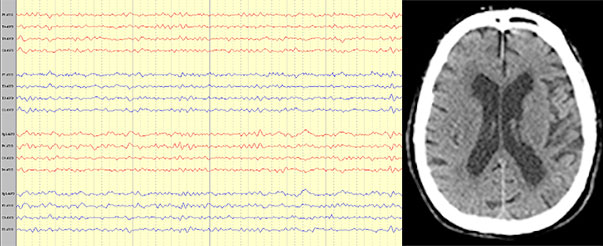
Figure 1.EEG showing non-specific slowing of the background rhythm and CT scan of the brain showing generalised atrophy.
Conclusion
Despite the fact that 48% of patients report adverse effects secondary to omeprazole ingestion, only a very small minority complain of neurological symptoms, the majority of which being headaches (3% of total side-effects).8 Neuropsychiatric symptoms including delirium have been reported in the literature9 and are also documented in the product literature. The summary of product characteristics (for Losec®)12 acknowledges that psychiatric symptoms including delirium can occur rarely, secondary to severe hypomagnesaemia in patients treated with proton pump inhibitors for at least 3 months. Case reports also report delirium secondary to hyponatremia in patients treated with proton pump inhibitors for at least 3 months.13 Notwithstanding this fact, the authors conducted a thorough literature search and did not find any case of documented omeprazole-induced delirium whereby sodium and magnesium levels are normal. In conclusion, physicians should not undervalue the possibility of documented omeprazole-induced non-organic psychosis. Earlier recognition and prompt cessation of the drug will avoid unnecessary investigations as well as reduce the length of hospital stay.
References
1. S.K.Inouye. Delirium in older persons. N Engl J Med 2006; 354:1157-65.
2. E.De Lange, P.F.M.Verhaak, K.Van der Meer. Prevalence, presentation and prognosis of delirium in older people in the population, at home and in long term care: a review. Int J Geriatr Psychiatry 2013; 28:127-34.
3. N.Siddiqi, A.O.House, J.D.Holmes. Occurrence and outcome of delirium in medical in-patients: a systematic literature review. Age Ageing 2006; 35:350-64.
4. Marcantonio ER. Postoperative delirium: a 76-year-old woman with delirium following surgery. JAMA 2012; 308:73-81.
5. E.G. Teneille. Delirium: A review. Can J Neurol Sci 2011; 38: 673-680.
6. A.G. Catic. Identification and Management of In-Hospital Drug-Induced Delirium in Older Patients. Drugs Aging 2011; 28 (9):737-718.
7. J. G. Heckmann, F. Birklein and B. Neundörfer. Omeprazole-induced delirium. J Neurol 2000; 247:56–57.
8. S. Fujiia, H. Tanimukaib, and Y. Kashiwagid. Comparison and Analysis of Delirium Induced by Histamine H2 Receptor Antagonists and Proton Pump Inhibitors in Cancer Patients. Case Rep Oncol 2012; 5:409–412.
9. Omeprazole Summary of Product Characteristics. August 2012.
10. D.D. Moyer. Terminal delirium in geriatric patients with cancer at end of life. Am J Hosp Palliat Care 2011; 28(1):44-51.
11. S.K. Inouye. Delirium in older persons. N Engl J Med 2006; Vol. 354 (11):1157-65.
12. Astra Zeneca AB Sweden. Losec Summary of Product Characteristics. Last revised February 2014. Accessed August 2014.
13. Z. Fireman, Y. Kopelman and S. Sternberg. Central Nervous system side effects after proton pump inhibitor treatment. J Clin Gastroenterol 1997;