
MR Imaging of EARLY Rheumatoid Arthritis and Spondyloarthropathy – Part I
by Pierre Vassallo
Rheumatoid arthritis (RA) and spondyloarthropathy are two groups of inflammatory joint disease. Detection of early inflammatory joint disease is not possible with clinical examination or plain radiography, which have been the main diagnostic methods in the past. Changes detected on plain radiography are those of chronic damage caused by these conditions rather that acute inflammation, which results in delay in diagnosis and often suboptimal outcomes in these patients.
RA is the most common inflammatory arthritis, affecting approximately 1% of the world’s population. In 25% of cases, non-articular soft tissues are also involved in the inflammatory process. RA results from inflammation of the synovial membrane (synovitis), with joints becoming swollen, tender and warm and stiff. Most commonly involved are the small joints of the hands, feet and cervical spine, but larger joints like the shoulder and knee may be affected. Multiple joint involvment (polyarthritis) is common and is typically symmetrical in distribution although not in early disease. Over the last two decades, significant improvement in its prognosis has been achieved owing to new strategies for disease management, the emergence of new biologic therapies (including tumor necrosis factor–blocking agents such as rituximab, abatacept, and tocilizumab) and better utilization of the conventional disease-modifying antirheumatic drugs. Furthermore the generalized use of standardized criteria for the evaluation of disease activity such as the American College of Rheumatology (ACR) improvement criteria and European League Against Rheumatism response criteria have proved useful for monitoring the disease course in daily clinical practice.
In contrast, spondyloarthropathy comprises a group of chronic inflammatory rheumatic diseases, including ankylosing spondylitis, reactive arthritis (Reiter syndrome), arthritis or spondylitis associated with inflammatory bowel disease, and psoriatic arthritis, as well as undifferentiated spondyloarthritis. These afflictions predominantly affect the axial skeleton, causing pain and stiffness; are seronegative for rheumatoid factor; and are often associated with the presence of human lymphocyte antigen (HLA)–B27. They are largely differentiated on the basis of clinical information and the distribution of radiographic abnormalities. Spondylarthropathy tends to have an asymmetric distribution when multiple joints are affected.
MR imaging has demonstrated greater sensitivity for the detection of synovitis and erosions than either clinical examination or conventional radiography and can help establish an early diagnosis of RA and spondyloarthropathy. It also allows the detection of bone marrow oedema, which is thought to be a precursor for the development of erosions in early RA and spondyloarthropathy as well as a marker of active inflammation. In addition, MR imaging can help differentiate RA from some clinical subsets of peripheral spondyloarthropathies by allowing identification of inflammation at the insertions of ligaments and tendons (enthesitis).
Magnetic resonance (MR) imaging has become the most recent innovation and the important change with respect to the previously established classification criteria. MR imaging can serve as a biomarker of disease activity, allows monitoring, and can provide guidance for the treatment of affected patients, and has become even more central to the care of these patients. Familiarity with the anatomy, anatomic variants, and physiologic joint changes is important for correctly interpreting findings and avoiding misdiagnosis.
The term early RA is not defined precisely in the literature. Most authors use the term to describe only disease duration of less than 1 year from the first episode of clinically detectable joint inflammation, although the duration of early RA varies widely between publications (up to 2–3 years in some series). Erosions, periarticular osteopenia, and cartilage loss are all known to occur within 2 years of the onset of RA in the absence of effective therapy. Radiography is not helpful for establishing an early diagnosis of RA, since fewer than 20–25% of patients initially present with erosions. Up to 30% of patients test negative for serum rheumatoid factor, and other pathognomonic features such as rheumatoid nodules usually appear late in the disease process. In addition, RA may start in atypical fashion. It can have a very sudden onset with marked systemic features such as fatigue, fever, and weight loss, or can manifest as polymyalgia rheumatica syndrome (pain and morning stiffness in the hip and shoulder girdles), oligo- or even mono-arthritis, or bilateral carpal tunnel syndrome. The extent of irreversible joint damage and disability will depend primarily on how much time has elapsed before satisfactory treatment is achieved. The effectiveness of management strategies designed to disrupt the development of RA and prevent the long-term effects of this disease depends largely on early initiation of treatment.
When imaging for RA, the hands are the most likely to be involved and usually symmetrically. However it is best to image the more painful hand since this is likely to produce more florid findings. Imaging should include coronal and axial T1-weighted, STIR or fat-saturated T2-weighted images and pre- and post IV contrast (Gadolinium DTPA) Fat-Saturated T1-weighted images using a high resolution flexible coil and covering all the wrist joints as well as the MCP and PIP joints since this is the most common pattern of distribution in RA.
Synovitis is the earliest abnormality to appear in RA. Normal synovial tissue that lines joint cavities, bursae, and tendinous sheaths is usually too thin to be visible on MR images. MR imaging signs of synovitis include synovial thickening, increased water content, contrast enhancement, or a combination thereof (Fig 1). Contrast enhanced T1-w MR images allow distinction between synovial hypertrophy and joint effusion. Fibrotic pannus, which is usually present in end-stage rheumatoid arthritis, may show poor or limited enhancement after the intravenous administration of gadolinium-based contrast material.
(to be continued)
Figure Legends

Figure 1. Synovitis in early RA of the wrist (6 months duration); patient had normal radiographic findings. (a) Coronal T1-w MR image shows extensive synovitis (arrows). On STIR
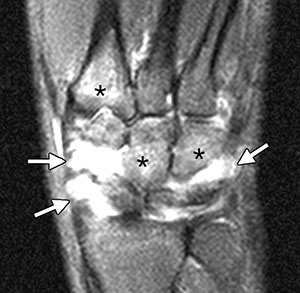
(b) and axial fat saturated T2-w
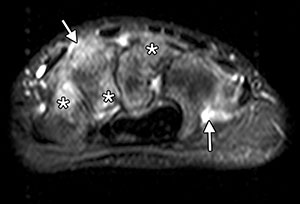
(c) MR images, the synovitis has high signal intensity (arrows). * indicate bone marrow oedema at the bases of the second metacarpal, capitate, and hamate bones.

(d) Sagittal contrast-enhanced fat-saturated T1-w MR image shows intense enhancement of the periscaphoid synovitis (arrows), in the area of bone marrow oedema in the scaphoid bone and in the base of the second metacarpal bone (*).