
Monitoring of Thyroid Function Tests in Hypothyroid Patients on Levothyroxine
Clayton J. Fsadni & Sarah Caruana Galizia
Abstract
The study aims to identify and recommend ways of improving thyroid function monitoring. Over a three month period, eighty-eight patients with clinical and subclinical primary hypothyroidism on long-term levothyroxine therapy were seen by GPs at the Chronic Disease Managment Clinic. The monitoring intervals of thyroid function tests for patients with controlled and uncontrolled primary hypothyroidism were benchmarked with the American Association of Clinical Endocrinologists guidelines.
The overall average compliance for clinical hypothyroid cases was 69% (n=15) and 40% (n=9) for the subclinical hypothyroid cases. In the clinical hypothyroid cases compliance was 71% (n=15) and 67% (n=14) for controlled and uncontrolled cases, respectively. In the subclinical hypothyroid cases compliance was 43% (n=10) and 35% (n=8) for controlled and uncontrolled cases, respectively. Knowledge of the guidelines amongst GPs should be increased especially when it comes to the management of subclinical hypothyroidism, and in cases of uncontrolled hypothyroidism in general. This is possible through better dissemination, availability and reinforcement of such guidelines.
Introduction
Primary hypothyroidism results from under-secretion of thyroid hormones from the thyroid gland. The most common cause of primary hypothyroidism is chronic autoimmune thyroiditis (Hashimoto’s Disease). Other causes include throidectomy, thyroid gland ablation with radioactive iodine, external irradiation, a biosynthetic defect in iodine organification, thyroid lymphoma and drug-induced. Signs and symptoms are generally related to the duration and severity of hypothyroidism, the rapidity with which hypothyroidism occurs, and the psychological characteristics of the patient. Hypothyroid patients usually present dry skin, cold sensitivity, fatigue, muscle cramps, voice changes and constipation.1
Increased thyroid stimulating hormone (TSH) values usually indicate hypothyroidism whilst decreased values usually indicate hyperthyroidism. This test has proved to be both sensitive and specific for hypothyroidism. An elevated TSH level with a normal free T4 level is referred to as subclinical hypothyroidism. It is important to note that patients with subclinical hypothyroidism may still have clinical symptoms.2 In general, hypothyroidism can be adequately treated with a constant daily dose of levothyroxine, usually with a single maintenance dose of 100-200 mcg.3,4
TSH levels are the best indicator of thyroid function and the best test for monitoring response to levothyroxine therapy.5 It has been found that adverse events related to replacement therapy with levothyroxine are more common in patients who do not receive the recommended monitoring.6 Therefore, monitoring of thyroid function tests (TFTs) has a role to gauge the thyroid function response to levothyroxine, ensuring the minimum effective dose at the least adverse drug effects.
Aims
• To evaluate the adequacy of thyroid function test (TFT) monitoring in patients with primary hypothyroidism that are on levothyroxine therapy.
• To recommend ways in which TFT monitoring can be improved.
Method
Setting and sampling
An audit was conducted in a Primary Care setting at Qormi Health Centre from July till September 2015. The reason for conducting the study solely at the Qormi Health Centre was that during the study period, the only Chronic Disease Management Clinic (CDMC) was located at that centre. All patients with clinical and subclinical primary hypothyroidism, that were on long term levothyroxine (for more than 3 months), were identified from the CDMC by the ten GPs that practice in this clinic. The cohort amounted to eighty-eight patients. The study excluded hypothyroid patients that had disturbances of hypothalamic-pituitary function and females that were pregnant. With regards to subclinical hypothyroid patients, only those with TSH levels > 10 micro IU/ml were considered, as data for patients with mildly raised TFTs is controversial.1
Hypothyroid patients, including those diagnosed with subclinical hypothyroidism, were identified by the GPs that regularly follow patients at the CDMC. For each patient, the ID number and date of visit of the patient were recorded by the GPs on a data sheet which was distributed prior to the commencement of the study. For each patient, iSOFT clinical manager was then used to identify the TFT results over the previous year. The time interval between TFT monitoring for controlled and uncontrolled thyroid function for both clinical and subclinical hypothyroid patients was recorded.
Standards
The standard criteria established by the AACE (last updated in 2012) are as follows:
1. Well-controlled subclinical hypothyroid patients (normal TSH) should have their TFT monitored every 48 weeks.
2. Patients with uncontrolled subclinical hypothyroidism or patients who experienced a change in levothyroxine dose should have their TFT checked every 6-8 weeks.
3. Well-controlled clinical hypothyroid patients (normal TSH levels) should have a TFT repeated at 24 weeks and the 2nd TFT at 48 weeks.
4. Patients with uncontrolled clinical hypothyroidism, or patients who experienced a change in levothyroxine dose should have the TFT repeated at least 6 weeks after a deranged TSH level, or dose adjustment, respectively.
Data Analysis
All data were processed using Microsoft Excel 2013. The data were then analysed by recording the TSH monitoring intervals for patients with subclinical/clinical hypothyroidism with normal/abnormal TFTs. Compliance with AACE guideline criteria was recorded for each category.
Ethical approval and consent
The study was approved by the Audit Committee and the Data Protection Act Committee. Consent was achieved from the Principal General Practitioner and Clinical Director of Primary Health Care.
Results
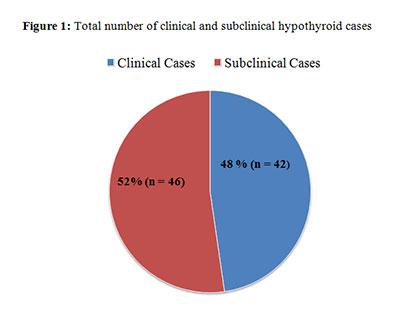
48% (42 from 88 patients) studied had clinical hypothyroidism, whilst 52% (n=46) had subclinical hypothyroidism (Figure 1).
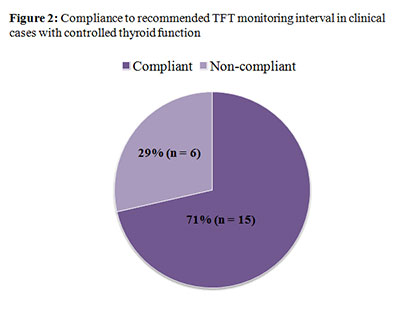
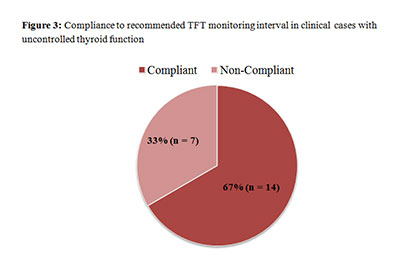
In controlled clinical hypothyroid cases 71% (n=15) compliance to the recommended TFT monitoring interval, as per AACE guidelines, was observed (Figure 2) whilst for uncontrolled cases compliance was 67% (n=14) (Figure 3).
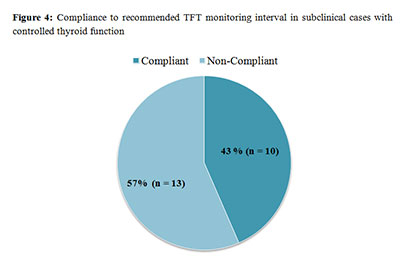
In controlled subclinical cases there was 43% (n=10) compliance to the recommended TFT monitoring interval, whilst for those with abnormal TFTs there was 35% (n=8) compliance to the recommended monitoring interval (Figures 4 and 5 respectively).
When considering both controlled and uncontrolled cases, the overall average compliance for clinical and subclinical hypothyroid cases were 69% (n=15), and 39% (n=9) respectively. This was achieved by calculating the mean of the compliance for controlled and uncontrolled cases in both clinical ((71% + 67%)/2) and subclinical hypothyroid ((43% + 35%)/2) cases.
Discussion
In this study all patients with hypothyroidism were on levothyroxine treatment. Since downward dose adjustment or even cessation of levothyroxine therapy may be required, T4 and TSH monitoring is necessary for the management of both clinical and subclinical hypothyroidism.
For both controlled and uncontrolled hypothyroid cases compliance to the thyroid monitoring guidelines was noted to be greater for patients with clinical hypothyroidism (69%) than for those with subclinical hypothyroidism (40%). The most probable reason for this is that physicians are more aware of thyroid monitoring frequency guidelines for clinical hypothyroid cases. Furthermore, physicians may have experienced difficulties in interpreting subclinical hypothyroid biochemical derangements and thereby in differentiating it from clinical hypothyroidism. Delayed monitoring was noted whenever physicians showed non- compliance in both patient categories with normal and abnormal TFT results. This is contrary to what is normally expected since uncontrolled hypothyroid cases require shorter interval monitoring times, hence a stricter monitoring approach.
The results show that physicians are not aware of the clinical importance of adequately monitoring subclinical hypothyroidism, with more importance being given to clinical hypothyroidism. Regular monitoring of TSH levels in primary care patients can be ensured through a computer-generated recall system with written notification to patients.7
Limitations
The main limitation of the audit was the small sample size which may have led to inaccuracies in the interpretation of the results. In most cases no documentation was found with regards to changes in levothyroxine dose, hence it was assumed that a change in dose was made with every deranged TFT result. Data was only collected by GPs working at the Qormi Health Centre, and hence the data may not truly represent compliance to the guidelines in patients attending other health centres. The audit did not assess the possible reasons for abnormal TSH levels, for example pregnancy, medication interactions and compliance to levothyroxine therapy.
Conclusion and Recommendations
This audit has shown that there is room for improvement when it comes to thyroid function monitoring, especially in cases of subclinical hypothyroidism. Physicians should be more aware of the biochemical derangements that correlate to subclinical hypothyroidism which will enable them to differentiate it from clinical hypothyroidism. Whilst excessive monitoring leads to unnecessary visits by patients and increased expenditure, on the other hand, delayed monitoring may lead to inaccurate dosing of levothyroxine and hence possibly increased adverse effects and/or ineffective thyroid function control.
In order to improve compliance to the AACE guidelines, it is recommended that they should be well-disseminated both at Mater Dei Hospital medical outpatients clinic and at health centres (where many patients have their thyroid function monitored). Knowledge of the guidelines especially amongst GPs can be increased by means of seminars and conferences given by endocrinologists. A downloadable PDA version and availability of the guidelines on KURA would also help to improve compliance.
References
1. Garber JR, Cobin RH, Gharib H, Hennessey JV, Klein I, Mechanick JI, et al. Clinical practice guidelines for hypothyroidism in adults: cosponsored by the American Association of Clinical Endocrinologists and the American Thyroid Association. Endocr Pract. 2012;18(6):988-1028. Erratum in: Endocr Pract. 2013;19(1):175.
2. Adlin V. Subclinical hypothyroidism: deciding when to treat. Am Fam Physician. 1998;57(4):776-80.
3. Orlander PR , Griffting GT. Hypothyroidism treatment and management. Medscape [online]. Available from http://emedicine.medscape.com/article/122393-treatment
4. Joint Formulary Committee. British National Formulary. No. 69. London: BMJ Group and Pharmaceutical Press 2015.
5. Stelfox HT et al. An evaluation of the adequacy of outpatient monitoring of thyroid replacement therapy. J Eval Clin Pract 2004;10:525-30.
6. Medsafe Eltroxin tablets datasheet. Available from: www.medsafe.govt.nz/profs/Datasheet/e/Eltroxin(new)tab.htm
7. Bretherick N. Monitoring the thyroid in general practice. Forum Research. 2011; 57-8. Available from: www.icgp.ie/assets/93/1793E8AC-19B9-E185-83AAC778DB059BE1_document/Thyroid_PAGE57-58.pdf