
Migraine
Anthony Galea Debono MD FRCP FRCPE
Consultant Neurologist & Senior Lecturer in Neurology
St Luke’s Hospital & Boffa Hospital
1. Epidemiology
Migraine is perhaps one of the commonest ailments afflicting mankind. Two of the most important studies about the prevalence of migraine are the American Migraine Studies 1 and 2. The first study was carried out in 1989 and the second was carried out in 1999. These studies showed that the prevalence of migraine remained the same overall. In 1989, 5.7% of the male population had migraine, while in 1999, the figure was 6.5%. The prevalence rates for women were 17.6% in 1989 and 18.2% in 1999. The diagnosis of migraine was based on the criteria established by the International Headache Society (IHS).
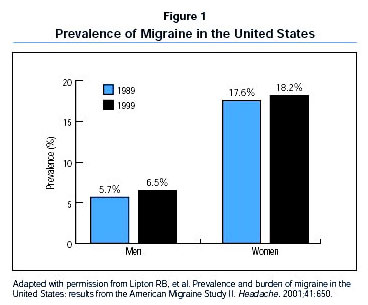
Migraine is approximately three times more common in women than in men.
Approximately 1 household in every 4 includes an individual who suffers from migraine.
2. Diagnosis
Unfortunately, migraine is one of the more frequently misdiagnosed conditions and this leads to inappropriate treatment.
The criteria established by the International Headache Society should help clinicians make a more accurate diagnosis.
Figure 2
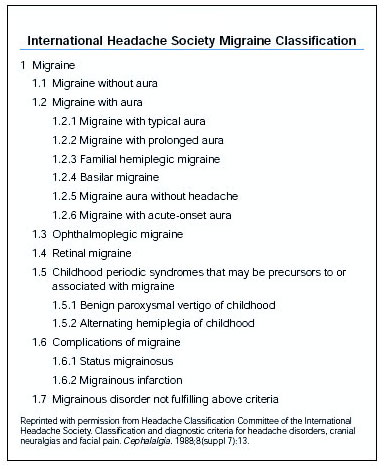
Essentially, the major forms of migraine are classified according to whether there is a preceding aura or not. The diagnosis of migraine is a clinical diagnosis, based on the history.
Tension Headache is often misdiagnosed as Migraine.
It is to be noted that Migraine and Tension Headache can co-exist in the same patient. Care should be taken to distinguish between the two.
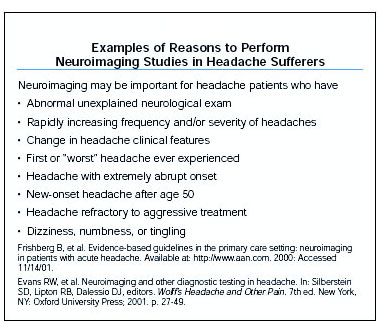
Neuroradiological investigations are not normally necessary.
Figure 3
Indications for neuroimaging
3. Genetic and Environmental Factors
Current evidence from family aggregation studies show that if patients suffer from migraine with aura, first degree relatives have a four-fold increase in risk.
If the patient has migraine without aura, the relative risk for first degree relatives is less. However the risk is still appreciably higher than that found in a normal population.
Current evidence would suggest that both genetic and environmental causes are important in the aetiology of migraine.
4. Acute treatment
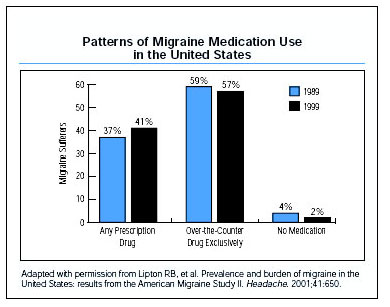
As both migraine with aura and migraine without aura are often self diagnosed, fewer patients tend to consult their Family Doctor or a Neurologist. Most patients self medicate with over the counter products. Around 60% of patients do well on such a regime (figure 4). Prescription medications are less often used.
Figure 4
The aims of Acute Treatment should include:
- Restoration to normal function as soon as possible;
- Optimization of self care;
- Cost effectiveness;
- Minimal or no adverse side effects.
Drugs which have been shown to be effective in well-designed, randomized clinical trials and which have yielded consistent satisfactory results include the following: Aspirin, Paracetamol, NSAIDS and the Triptans.
Drugs which were shown to be effective in at least 1 double-blind controlled trial and where there is a clinical impression of benefit, include the anti-emetics Metoclopramide and Prochlorperazine.
The evidence for Ergotamine efficacy is conflicting. This drug should be avoided because of overuse and because of the risks of potential severe side effects.
5. Preventive Treatment
Individuals who experience frequent and disabling attacks may not be adequately managed by acute therapy alone. Drug prevention therapy will help to reduce the frequency, severity and duration of the migraine attacks in this group. It could help reduce the disability associated with attacks and reduce the risk of worsening the migraine condition by the overuse of acute medications.
Preventive treatment is to be considered in the following situations:
- Migraine attacks which recur and interfere with daily functioning;
- Frequent migraine attacks, occurring more than three times per month;
- When acute medications are not well tolerated or ineffective;
- When there are contraindications to acute medications.
A number of drugs are used as prophylaxis. These include Amitriptyline, Valproate and Methysergide. The efficacy of these drugs has been shown in multiple well-designed randomized clinical trials.
There is some evidence from clinical trials that Gabapentin, Atenolol and Verapramil are also effective.
Topiramate is a recent addition to the armamentarium.