
Maximising ophthalmic theatre time – Part II
Paola Bonanno, Maria Agius, Franco Mercieca
Discussion
Currently the allocated theatre time for this particular firm is that of five and a half hours per week. An extra average of four hours per week are gained by using theatre time on weekends or public holidays. From this in-house audit an average of 92% of the available theatre time, during the months under study, was used while the remaining 8% was ‘un-utilised’. In interpreting the latter percentage one has to take into consideration any last minute cancellations which resulted in wasted theatre time. In the absence of Pre-operative Assessment Clinics (POAC) held 1 to 2 weeks ahead of the scheduled date of surgery we still have to pre-assess our patients due for surgery under local anaesthesia on the day of the surgery. Since most patients would have been waiting for several years for their eye surgery, both their ocular status and general health may have altered making them unsuitable for surgery. Therefore the setting up of Pre-Operative Assessment Clinics would significantly improve our efficiency and safety. Patients would also be psychologically better prepared for surgery knowing that all the necessary tests have already been performed on a previous date and would not have to endure a last minute test to verify their fitness for surgery. The POAC would also create a pool of patients who are already prepared and tested, whom we could call on the day to fill up any possible last minute cancellations.
According to the Bevan report,1,2 the UK’s NHS Management executive recommends 90% utilisation of theatre time, which compares reasonably well with the percentage utilisation of theatre time quoted in our study. However one has to note that for the sake of this study we have allocated a fixed amount of time for any particular procedure to be completed. Therefore it was assumed that these procedures were all routine and uncomplicated, all surgeons in this firm were of equal speed and all patients were fully co-operative (referring to local anaesthesia patients). It was also assumed that there was never any delay in bringing patients from the ward and that on every session there was a full compliment of nursing staff in the operating theatre. An assumption has also been made that no teaching of junior doctors was carried out. Therefore if all these factors are taken into consideration, one immediately realizes that the theatre time efficiency is actually much higher.
is study the duration between operations i.e. the turnover time has been estimated as being 2 minutes. It often means that the doctor or nurse has to wheel the patient out of theatre before getting the next patient in. Better use of health assistants or other auxiliary staff may lead to a faster turnover leading to better use of the limited theatre time.
In order to maximize usage of theatre time, our patients are encouraged to have their cataract surgery under local anaesthesia (LA) unless patients have a communication deficit due to their mental status, language barrier or hearing deficit.
Having eye surgery under general anaesthesia (GA) increases the onus on the anaesthetic department, minimally increases the anaesthetic risk on patients and leads to more wastage of precious theatre time. Simple mathematics confirm that performing cataract surgery under LA will double the surgical output when compared to being carried out under GA. In fact it is a policy of this firm to group all patients requiring surgery under GA on one operating theatre day per month and all other lists are dedicated for LA only, in order to improve the efficiency as much as possible. Nowadays the LA method of choice is the SubTenon technique, in which a blunt curved cannula is used without the need of any needles. Therefore the LA is very well-tolerated, safe, effective and reproducible. 3
In the quest to decrease the cataract waiting list the authorities are all the time endeavouring to increase the number of cataract surgeries. In fact this study shows that from the official allocated hours, 64% is dedicated to cataract surgery alone with the rest allocated to other types of ophthalmic interventions. While a patient with a cataract can wait, without any significant detriment on the eventual surgical outcome, the same cannot be said for patients requiring a retinal detachment operation or glaucoma surgery. Patients who suffer from the latter conditions take priority on cataract patients. In fact almost 7% of theatre time was used for glaucomarelated surgery. 22 corneal transplants were also carried out by this firm in 2009. The latter were all performed before or after the allocated theatre time in order not to negatively impinge on the cataract waiting list. Squint surgeries are usually also grouped in separate sessions in order to streamline the surgical output.
Regular use of topical local anaesthesia instead of sub-Tenon’s infiltration of anaesthesia can the hasten duration of cataract surgery and allows patient to recover visual acuity rapidly after surgery.4 However topical anaesthesia is associated with more discomfort during surgery than sub-Tenon’s anaesthesia. Therefore currently, the latter remains the preferred choice for this firm.5
Most cataract patients have bilateral disease and this would imply that if the waiting time for a cataract procedure is 4 years then they have to wait a minimum of 8 years till completion. Therefore the possibility of simultaneous bilateral cataract surgery (SBCS) is a notion one should consider seriously even though, as evidenced in a consultation forum6 involving international experts in 1997, SBCS remains controversial. Several recent reports highlight the safety factor of SBCS7,8,9 due to the advent of sutureless cataract surgery. The potential advantages of SBCS are definitely not insignificant. SBCS reduces the time spent by patients and medical staff in the overall process. Some advantages include performing one surgical event which is shorter than two put together, fewer postoperative visits, reduced administrative paperwork, less temporary disability and sick leave and reduced reliance on the support of family and friends. In this regard, the true economic saving of SBCS go far beyond one can imagine. Healthcare professionals often underestimate the emotional stress or physical hardship that surgery and postoperative period entail for certain patients. For these individuals eliminating a second intervention may be desirable. In his editorial of the British Journal of Ophthalmology10, Chang D F concludes that ‘in any healthcare system where limited resources may impose rationing or lengthy delays in elective surgery, SBCS might be the best way to safely extend the benefits of cataract surgery to as many eyes as possible’. Despite all this, ‘in analysing the downside to SBCS, the most important complications to consider would be those occurring during the early postoperative period. Some, such as endophthalmitis, are vision threatening and others, such as refractive surprise, are not. Some, such as moderate corneal oedema or toxic anterior segment syndrome, are temporary. All of these complications could have altered the timing or outcome of the second operation.’10
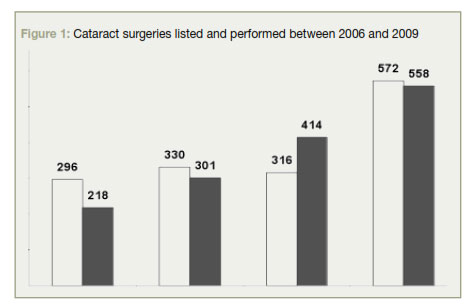
In 2009 this firm carried out 572 cataract procedures which means an 81% increase from the previous year. Only 48% (275) were performed during the allocated theatre time while 52% (297) were carried out during weekends and public holidays. The usage of theatre time during weekends is, in agreement with the anaesthetic department, dedicated solely to LA patients except in case of emergency. Therefore this extra theatre time is mainly dedicated to cataract surgeries which amounted to 85% of the utilised theatre time. The reason why the percentage utilization of extra theatre time increases to 94.95% (compared to 89.25% in the allocated hours), is due to the fact that lists on weekends/ public holidays run much smoother, primarily driven by the presence of a full compliment of the nursing staff. This is in stark contrast to weekdays when nurses are stretched to the limit.
The drastic increase in the number of cataract surgeries performed in 2009 was due to the fact that allocated theatre time was extended on Mondays by 2 hours and longer lists on weekends/public holidays were possible. Furthermore, in 2008 there was a drop in the number of cataract surgery performed, possibly due to the migration to Mater Dei Hospital.
Although 572 cataract operations were carried out in 2009, 558 patients were listed in the same period for the same procedure. Therefore the benevolent action to work on weekends did not lead to a decrease in the waiting list, but merely was just enough to cope with the current demand. In fact 2009 was the first year that the supply was equivalent to demand while in the past we were listing a higher number of patients when compared to surgeries. From the sample months that were analysed it results that in the allocated theatre time only 6 cataract operations were performed each week while 12 were carried out on every list in the extra theatre time. The latter was possible since only LA patients were carried out on weekends which streamlined the output considerably.
Mr Mercieca’s current waiting list is around 1700 patients for cataract surgery. Thus if his firm is allowed an extra session of 5 hours per week which would be dedicated solely to LA cataract operations, an average of 10 extra cataract operations would be performed leading to a decrease in the waiting list by around 500 a year. This would be correct if we assume that the demand for cataract surgery remains the same when in fact we expect the opposite as seen in Figure 1. Due to the ever increasing aging population and increasing patients’ trust in the success of this life-enhancing surgery, the demand for cataract surgery is bound to continue to increase. This could mean that it may take us at least five years to bring the waiting list to acceptable levels.
Conclusions
In order to maximise the usage of our current allocated and extra theatre time, the authors suggest:
1. The setting up of Pre-Operative Assessment Clinics in order to streamline our surgical output and reduce to a minimum the theatre time wastage.
2. Encourage more patients to have their eye surgery under local anaesthesia
3. Proper help from auxiliary nursing staff in transporting patients in and out of operating theatre and even to and from Ophthalmic Ward.
4. Consider the possibility of Simultaneous Bilateral Cataract Surgery as a way to economise on our health resources
However it is quite obvious that maximising on our theatre time would never address the problem of our unacceptably long waiting lists. From our study it transpires that the only way to significantly positively impact on the waiting list for cataract surgery is to have an additional operating theatre in parallel with our current setup dedicated solely to cataract surgery under local anaesthesia, ideally led by one or two ophthalmic surgeons.
After all the reason why nowadays we have such an unacceptable long waiting list is entirely due to the fact that cataract surgical results have improved tremendously. This has led to an exponential increase in the demand for the surgery which has not been met by the supply, leaving a lot of patients waiting too long a time for this quality of life enhancing-surgery.
In fact 2009 was the first year that the supply was equivalent to demand while in the past we were listing a higher number of patients when compared to surgeries.
Acknowledgments
Acknowledgements go to Mark Debono and Dr Alexandra Distefano for their assistance in collating data required for this research.
References
1. Caleb D Mpyet, FWACS. An Audit of the Use of Ophthalmic Theatre Time. Community Eye Health 2002; 15(44):623. 2. NHS Management Executive. The Management and Utilisation of the Operating Department (the Bevan Report). London: HMSO; 1989. 3. Roman S, Sit D, Boureau C, Auclin F, Ullern M. Sub-Tenon’s anaesthesia: an efficient and safe technique. Br J Ophthalmol 1997; 81(8): 6736. 4. Kershner RM. Topical anaesthesia for small incision self-sealing cataract surgery. J Cataract Refract Surg 1993;19:290-2. 5. Chittenden HB, Meacock WR, Govan JAA. Topical anaesthesia with oxybupricaine versus sub-Tenon’s infiltration with 2% lignocaine for small incision cataract surgery. Br J Ophthamol 1997; 81:288-90. 6. Masket S, ed. Consultation section. Cataract surgical problem: under what conditions do you perform/consider bilateral simultaneous cataract extraction with intraocular implantation. What special precautions do you take/advice when considering bilateral surgery? J Cataract Refract Surg 1997; 23:1437-41. 7. Smith GT, Liu CSC. Is it time for a new attitude to simultaneous bilateral cataract surgery? Br J Ophthalmol 2001; 85:1489-96. 8. Totan Y, BayramlarH, Cekic O, et al. Bilateral cataract surgery in adult and pediatric patients in a single session. J Cataract Refract Surg 2000; 26:1008-11. 9. Konkanen M, Kaipianinen S. Simultaneous bilateral cataract extraction: a positive view. J Cataract Refract Surg 2002; 28:2060-1. 10. Chang DF ed. Simultaneous bilateral cataract surgery: An idea whose time has come? Br J Ophthalmol 2003; 87:253-4.