Maximising ophthalmic theatre time – Part I
Paola Bonanno Maria Agius Franco Mercieca
Abstract Aim:
To establish whether the available ophthalmic theatre time is being used efficiently and to find ways how to improve our surgical output and reduce the waiting list.
Methods:
All ophthalmic surgeries under the care of Mr Franco Mercieca carried out in Theatre 13 in the sample months of May and October 2009, were retrospectively analyzed. Average times were estimated for all types of ophthalmic procedures. The total number of cataract operations and patients listed for surgery were noted from beginning of 2006 till end of 2009.
Results:
In 2009, this firm has carried out 572 cataract operations, 81% increase from 2008, of which 52% were performed on weekends and public holidays. The theatre usage time in the sample months under study was 89.25% on weekdays and over 94% on extra sessions. Theatre time wastage was an average of 8%, half of which being due to cancellations on the day. On average over 71% of our theatre time is used for cataract surgery.
Conclusions:
In order to maximize our theatre time efficiency, we need to set up a Preoperative Assessment clinic and encourage more patients to have their surgery under local anaesthesia. To reduce the waiting list the need for a parallel theatre dedicated solely to cataract surgery under local anaesthesia is of paramount importance. Key words: Local Anaesthesia, PreOperative Assessment Clinic, Theatre Time.
Introduction
There is currently much talk among patients, healthcare workers and politicians about the long waiting list for cataract surgery at Mater Dei Hospital (MDH). The way patients are affected by the waiting time for this surgery has important clinical, public health and health policy consideration.
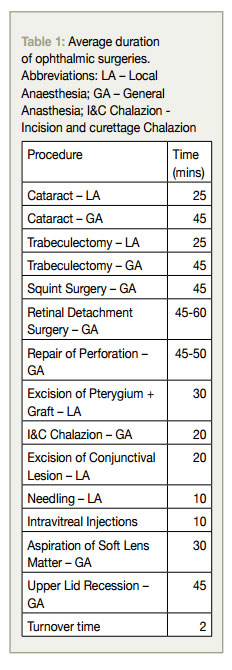
During the past decade, phacoemulsification has largely replaced large incision extra-capsular cataract extraction. The phaco incision is small and self-sealing allowing the surgery to be completed without sutures. This provides rapid visual rehabilitation, better wound stability and excellent postoperative astigmatic control.1-4 Cataract surgery has a low complication rate and is a relatively quick procedure (Refer to Table 1) with the majority of surgeries being done under local anaesthesia. All this is generating considerable improvement in the quality of life of patients who are treated. The demand for the surgery is therefore high and the Ophthalmology Department at MDH, given the constraints of limited resources, continuously struggles to meet these demands.
The number of cataract surgeries performed in Malta increased by almost 44% in 2009 when compared to the number performed in 2008.5 This was achieved by better usage of available theatre time and by performing extra lists on weekends and public holidays. Almost everyday from Monday to Sunday at Mater Dei Hospital there is a cataract surgery list. Yet this does not seem to be enough to meet the demands and the waiting list remains very long.
Aim
The aim of this audit is to establish whether the available ophthalmic theatre time is being used efficiently and to determine ways how this may be improved in order to decrease the cataract waiting list.
Method
All the elective and emergency major ophthalmic surgeries under the care of Mr. Franco Mercieca that were listed on the register of Ophthalmic Theatre 13 in the months of May 2009 and October 2009 were retrospectively surveyed. These months were chosen to make up for any seasonality factors and to make the assessment on two independent points in time in the same year.
All l ophthalmic surgeries carried out in the adjacent theatre 15 were excluded from this study since these were all minor operations including mainly various lid procedures and intravitreal injections.
The theatre time allocated to the firm is every Monday between 8.30am and 2.00pm. Extra theatre time is used optionally on Saturday and/or Sunday of any week when the respective consultant is on-call. The theatre time used on these days is between 8.30am and 12.30pm.
For the purpose of this study a case was considered to have started at the point in time when the patient is wheeled into the Operating Theatre (OT) and ended once the patient has been wheeled out. The average times estimated in this research include the following steps: Wheeling in the patient to the OT, checking patient details/ file, checking intraocular lens (IOL) power (where applicable), lying patient on operating table, administration of anaesthesia (whether local or general), scrubbing, draping, operating time, removal of drapes, reversal of anaesthesia (in the case of general anaesthetic), and eventual wheeling out of patient from OT. Turnover time – the time interval between the end of one case and the beginning of the next one – is not included in the estimates for each procedure. Table 1 indicates the average duration of the procedures. The table distinguishes the average operating time for surgeries performed either under Local Anaesthetic (LA) or General Anaesthetic (GA).
Note was also taken of the number of cataract surgeries that were cancelled on the day of the procedure and the reason of cancellations. The monthly total number of cataract performed and those booked on the waiting list from Ophthalmic Outpatients for the period between January and December 2009 was obtained from a network database available to the ophthalmic theatre nurse in charge. This data was compared to the preceding years till 2006.
Results
Operating Time availability
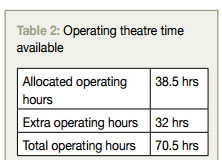
Table 2 highlights the operating time available to the firm under study during the research period including the regular time allocated and the additional optional hours used by the operating consultant. The number of regular operating days available in the period under study was of 7 (Mondays in the months under study) while the number of optional operating days used by the operating consultant was 8 (Saturdays and/or Sundays in the months under study).
Allocation of Operating Time
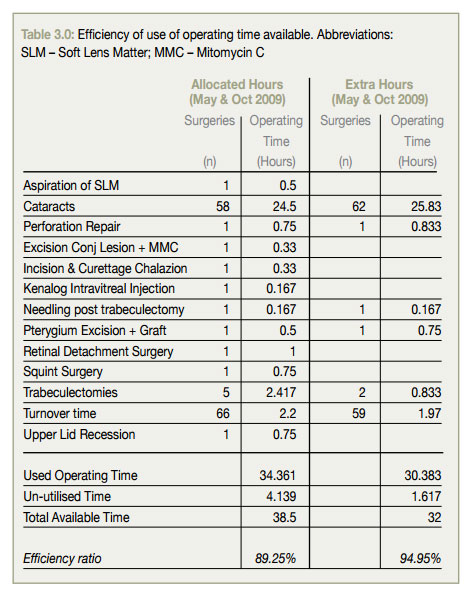
An important consideration for this study is the fact that while much importance is given to the cataract surgery waiting list in the media and amongst the administration, the operating theatre time has also to be used for other ophthalmic surgeries. In the data presented below in table 3.0 we analyse the share of operating time allocated between Cataract surgeries and other surgeries. One will note that circa 6% of the operating time available is wasted in necessary Turnover Time.
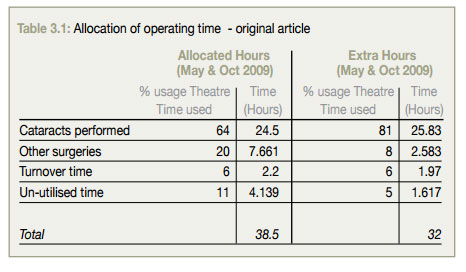
This data clearly indicates that the majority of the available operating theatre time – whether during allocated hours and extra hours – is dedicated to cataract surgeries, as shown in Table 3.1. In fact from these sample months, on average 71% of the total available theatre time is used for cataract surgery. While in the allocated theatre time this amounts to 64%, the percentage usage time for cataract surgery goes up to 81% during weekends or public holidays.
The ‘Other’/Un-utilised time shown in Table 3.1 represents the remaining theatre time which was could not be availed of or because it was used up for various other activities. This amounts to an average of 8% of the total available theatre time. Up to 4.7%, which amounts to around 3.3 hours, was not utilised due to last minute cancellations which was equally distributed between patients not turning up for surgery or found to be medically unfit on the day. The remaining 3.3% of this theatre time was taken up by complicated surgery, teaching ophthalmic surgery to juniors or delay in bringing patients from ward.
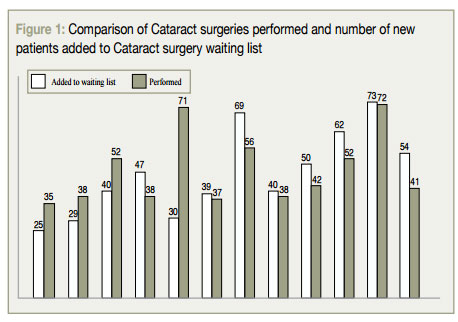
Surgeries performed vs Patients added to waiting list
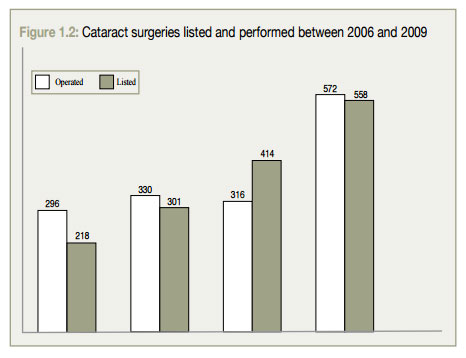
An important aspect of this study is the understanding of the number of new patients added to the waiting list for cataract surgery in contrast with the surgeries being performed with a view to reduce the number of patients on such list. Figure 1.0 below shows this comparison for the 12 months under study. It does not necessarily reflect the impact on the total waiting list but gives an indication of the regular number of new patients added to the waiting list month on month. Therefore in total 558 patients were listed for cataract surgery and 572 were operated on in 2009 under the care of Mr Franco Mercieca.
When compared to previous years, in 2009 there was a significant increase in the number of cataracts performed, as seen in Figure 1.1 with the main contribution being the work performed on weekends or public holidays. The percentage of the cataracts performed during extra theatre hours out of the total performed has increased exponentially from a mere 18% in 2006 to 52% in 2009. In 2008 we had a dip in total number of cataract surgeries performed (316 vs. 330 in 2007).
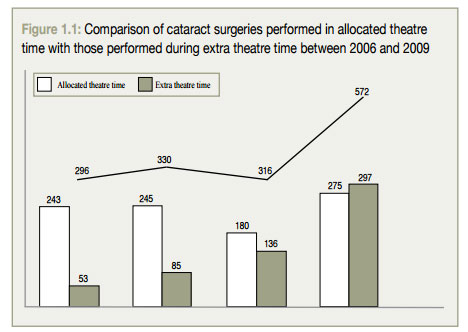
Figure 1.2 shows the number of patients who were listed for cataract surgery from 1st January 2006 till 31st December 2009 This illustration clearly shows how the demand for surgery has progressively increased over the three years analyzed.