
Mammographic Technology used for Breast Cancer Screening
Pierre Vassallo
Breast cancer, the most common cancer in women (1 in 8 women develops breast cancer), has generated considerable interest in the literature with the result that Breast Cancer
Screening Programmes have become the norm in developed countries. The aim of these screening programs is to achieve early detection of breast cancer in women who have not yet developed any symptoms. Such early detection would allow early treatment, which is necessary to achieve a good treatment outcome. It has been shown that treatment of early cancer results in cure in 98% of cases, while late cancer detection results in a poor outcome.
Early breast cancer detection depends on the accuracy of the equipment used and on training and experience of the specialists involved. Equipment accuracy and consequently image quality play a very important role as specialist training and experience do not compensate for poor image quality. There is considerable scientific evidence confirming the advantages of digital mammography over conventional film-screen mammography.
Film-screen mammography uses a chemically processed film to record images of the breast. On the othr hand, there are two different technologies used in digital mammography, computed radiography (CR) or full-field digital mammography (FFDM).
CR is a technology that obtains an image of the breast through exposure of a fluorescent plate, which is then scanned in a dedicated laser scanner to obtain a digital image of the
breast (Fig 1).
In contrast, FFDM technology uses an array of tiny solidstate electronic detectors embedded in the base plate of the mammography machine; the image of the breast obtained
by these tiny detectors is transferred directly to a specialised computer workstation for viewing (Fig 2).
CR uses an intermediate step in processing, namely the fluorescent plate; this significantly degrades image quality. FFDM, a significantly more expensive technology, obtains
images that are far superior to CR mammography (Fig 3).
FFDM has consistently been shown to be more accurate for detecting cancer than CR or conventional film-screen technology and is now considered the gold standard of mammography. In addition, FFDM uses 25-65% less radiation and is therefore much safer than other technologies. FFDM breast cancer screening has a high detection rate for
cancers particularly those containing calcifications (Fig 4a), most of which represent an early-stage cancer known as ductal carcinoma in situ (DCIS). Microcalcifications are defined as calcifications each measuring ≤0.5mm in diameter, and are particularly suspicious when >5 in number within an area ≤1cm in diameter, especially when distributed in a linear and branching (ductal) pattern and when they have a fragmented in a dedicated laser scanner to obtain a digital image of the breast (Fig 1).
In contrast, FFDM technology uses an array of tiny solidstate electronic detectors embedded in the base plate of the mammography machine; the image of the breast obtained
by these tiny detectors is transferred directly to a specialised computer workstation for viewing (Fig 2).
CR uses an intermediate step in processing, namely the fluorescent plate; this significantly degrades image quality. FFDM, a significantly more expensive technology, obtains
images that are far superior to CR mammography (Fig 3).
FFDM has consistently been shown to be more accurate for detecting cancer than CR or conventional film-screen technology and is now considered the gold standard of
mammography. In addition, FFDM uses 25-65% less radiation and is therefore much safer than other technologies. FFDM breast cancer screening has a high detection rate for
cancers particularly those containing calcifications (Fig 4a), most of which represent an early-stage cancer known as ductal carcinoma in situ (DCIS). Microcalcifications are defined as calcifications each measuring ≤0.5mm in diameter, and are particularly suspicious when >5 in number within an area ≤1cm in diameter, especially when distributed in a linear and branching (ductal) pattern and when they have a fragmented appearance. Microcalcifications may be very subtle (Figure 4b) and should raise clinical suspicion even at this stage. The visibility of microcalcifications is improved on FFDM compared with CR and film-screen mammography (Fig 5).
Invasive breast cancers, which are more advanced than DCIS, may also contain calcifications. In fact, around 35% of cancers detected on the basis of the presence calcifications are
invasive breast cancers.
Invasive cancers detected on the basis of calcifications in population-based digital mammographic screening also tend to be smaller (median, 7 mm) than those detected on the basis
of mass (median, 14mm), architectural distortion (median, 15mm), or combinations of both features (median, 17mm).
In addition, invasive cancers detected through the presence of calcifications noted on FFDM share the same degree of aggressiveness as those detected on CR and film-screen
mammography; in other words, we are not detecting less aggressive and maybe less significant cancers with FFDM. Nevertheless, the calcification-based detection rate for invasive
cancers in population-based screening is higher with FFDM than with CR or film-screen mammography.
The improved image quality of FFDM does not contribute only to detection of breast calcifications. Subtle areas of architectural distortion are also better seen and are often the
only sign of early malignant disease (Fig 6).
In summary, mammography is a valuable tool in the detection of early breast cancer and is our primary modality in breast cancer screening. The accuracy of mammographic
technology however, varies depending on the method used. FFDM performs significantly better and has become the gold standard for use in breast cancer screening. CR and film-screen mammography although still widely available and in common use, should be replaced by FFDM as these technologies no longer meet the standards expected in today’s clinical practice.

Figure 1a: CR mammography machine takes a cassette containing a fluorescent plate in the cassette holder (arrow).

Figure 1b. The CR laser reader withdraws the fluorescent plate from the cassette and scans it.

Figure 2: FFDM machine contains an array of micro detectors in the base plate (arrow).
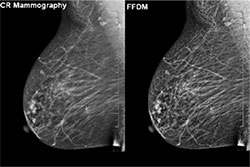
Figure 3: Comparison of CR versus FFDM: noted the sharper and more detailed image obtained by FFDM compared to CR.
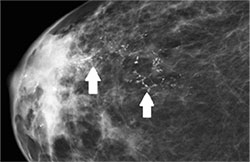
Figure 4a. Obvious microcalcifications distributed in a linear and branching pattern (arrows).
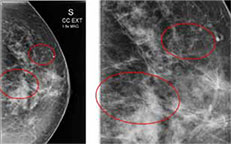
Figure 4b. More subtle fragmented microcalcifications in early DCIS (circles).
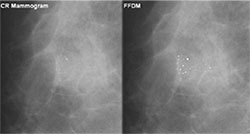
Figure 5: Comparison of microcalcifications seen on CR versus FFDM.

Figure 6. Very subtle early invasive ductal cancer detected through minimal architectural distortion (arrow) on FFDM. Th