
Intestinal Allergy: Food hypersensitivity in infancy and childhood
by Thomas M Attard
Gastrointestinal symptoms are frequently attributed to food hypersensitivity both by patients and increasingly by the medical community. Indeed, up to 35% of the general population in Western countries think they have food allergy1 although this is objectively confirmed in only 1-2% of the population.2 The incidence of food hypersensitivity appears to be on the rise, in parallel with the overall rise in atopic disorders over the last 30-40 years and concurrent with a decline in infectious disorders. This has lead to the emergence of the ‘hygiene hypothesis’ which raised awareness of the role of microbes and their products in immune regulation; more recently, this has prompted important observations on the impact of beneficial bacteria (probiotics) in the prevention of allergic processes.
The mechanisms underlying food hypersensitivity are complex and only partially understood: the atopic individual appears susceptible to a variety of allergic processes. This is in part a result of disordered mucosal immune function including IgA deficiency, increased epithelial permeability allowing the migration of larger, allergenic proteins over a more ‘porous’ interface and, as noted above, disordered epithelial microbial interaction. There are important differences in the cellular patterns of immune responsiveness to potential allergens in atopic compared with non-atopic individuals. These differences are based on both genetic factors, reflected by the clustering of atopic diseases in families, and the modulation of the immune system by extraneous factors including the intestinal flora (microbiome).3 The latter is supported by observations that children born by caesarean section have a different microbial profile in the large intestine and are more susceptible to milk allergy,4 and that probiotics exert a beneficial effect in childhood atopic eczema. Milk allergy is, on the other hand, less common in exclusively breast fed infants.5
Clinical Scenarios of Food Hypersensitivity
Food hypersensitivity in infancy:
Cows milk allergy (CMA; milk-soy protein intolerance, allergic enterocolitis) is a relatively common disorder in infancy; it appears to decrease in prevalence with age and affected infants are very likely to eventually outgrow it by the second year of life. Children with CMA are however at risk of other atopic disorders including asthma, hay fever and eczema (‘atopic march’) later in life. Affected infants typically present with gastrointestinal or skin manifestations in the first weeks in life. Gastrointestinal symptoms can run the gamut of irritability which overlaps with colic, severe reflux-type emesis, poor intake and failure to thrive, and colitis, including bloody diarrhea. Typical atopic dermatitis is also common.
Some misconceptions on CMA stem from confusion with lactose intolerance as discussed elsewhere. CMA is a clinical diagnosis and cannot rest on a single laboratory test. It is noteworthy that non-IgE-mediated allergic reactions are common in CMA so RAST testing is of very limited usefulness. In cases with severe manifestations, including hematochezia and hypoalbuminemia, endoscopy including colonoscopy may show patchy eosinophilic enteritis. It is also important to appreciate that breastfed babies, although far less likely, can still be affected through passage of allergenic epitiopes of cows milk in the maternal diet passing intact through breast milk.6 A strict milk and dairy exclusion diet in the breastfeeding mother is probably the best approach since persistent excretion of cows milk protein in maternal breast milk will delay symptom resolution, even though many parents find adherence to the diet particularly stressful. Although traditionally a switch to soy-based formula was advocated, since allergic infants can sensitize to soy in one third to half the time, management guidelines currently recommend a switch to a hypoallergenic, completely hydrolyzed formula.7,8 More severe cases may warrant an elemental, or amino acid-based formula, and in infants who refuse to eat or who have a persistent poor weight gain, nasogastric drip feeds may be used.
Food hypersensitivity in the older child and young adult
Food allergies in the older child include both IgE mediated and IgE independent mechanisms. In general IgE dependent reactions more closely follow allergen exposure and include more systemic cutaneous symptoms such as hives. Gastrointestinal upset includes cramps, nausea, diarrhea and fecal urgency. T-cell mediated reactions may not involve IgE production and are usually more restricted to gastrointestinal manifestations in their presentation. The symptoms of food allergy in the older child overlap with the clinical presentation of functional abdominal pain in childhood and irritable bowel syndrome (IBS) in adults.9 In the older child, unlike the infant with CMA, food hypersensitivity is an unlikely explanation for gastrointestinal hemorrhage or unexplained weight loss. This is a clinical diagnosis, sometimes supported by response to an empiric food exclusion diet although the sometimes long interval (weeks) between exclusion and clinical response needs to be explained to the parents and patient. Liaison with an experienced dietician is desirable insofar as strict exclusion of multiple allergens is extremely time consuming and stressful to some families. In some patients the diagnosis can be supported by gastroscopy and colonoscopy with biopsy that may show eosinophilic enteropathy in a patchy distribution and can rule out other etiologies including celiac disease and inflammatory bowel disease (IBD). Management rests with long term exclusion of allergen exposure. Pharmacologic therapy is limited; sodium cromoglicate,10 montelukast11 and ketotifen12 have all been used with variable success. Immunotherapy, including oral desensitization, has not yet been established beyond experimental protocols in the treatment of food allergies in childhood.13
Eosinophilic Esophagitis (EE)
A more recently recognized pattern of allergic enteropathy is eosinophilic esophagitis. Although initially described in children, it is now also established as an adult diagnosis.14 Patients with EE typically present with vague, upper gastrointestinal symptoms which overlap with gastroesophageal reflux disease.15 Both pain on swallowing as well as a sensation of food getting stuck (dysphagia and odynophagia) are common. Food bolus impaction in a previously asymptomatic individual is a classic clinical presentation. The patient’s background including family history may suggest atopy although not necessarily food allergy. The hallmark of EE is the persistence of symptoms despite maximal medical treatment with associated characteristic endoscopic – histopathologic findings (Figure 1). Indeed, EE is over-represented in cohorts of patients with esophagitis refractory to surgery (fundoplication).16 The treatment for EE includes both an intensive exclusion diet that is usually empirically based (six-food elimination diet; SFED), oral fluticasone as well as other systemic antiallergic agents. Continued surveillance, including endoscopy is encouraged because of concerns regarding long term sequelae including scarring.
Celiac Disease
Although not following the classic paradigm for a food hypersensitivity or allergic disorder, celiac disease is an environmentally triggered autoimmune disorder which shares several features with intestinal allergies. An in-depth discussion of celiac disease is beyond the scope of this review but it is worth reiterating that several reviews have highlighted the significant burden of undiagnosed celiac disease in our society. A recent review of the literature suggests that in several Mediterranean countries, amongst the low-risk and general population the prevalence of celiac disease identified through serologic screening ranges from 0.14% – 1.3%.17 The increasing incidence of celiac disease appears to parallel the presentation of more atypical clinical presentations of the disease. It is reasonable to consider and discuss serologic celiac screening (total serum IgA, anti-tTG IgA, IgG) in a broad gamut of clinical scenarios including apparent food hypersensitivity.
Milk Allergy or Lactose Intolerance?
Lactose intolerance is often confused with milk allergy, or more confusingly the two are hybridized as milk intolerance (Figure 2). Lactose intolerance refers to a condition of relative or absolute intestinal lactase deficiency; this brings about maldigestion of foods containing lactose, notably dairy. Undigested lactose is osmotically active and is fermented by endogenous bacterial flora resulting in diarrhea, gas and typically spasmodic abdominal cramps. Symptoms usually follow half an hour to several hours of exposure. Although lactose intolerance can be diagnosed through breath hydrogen testing a clinical diagnosis is usually sufficient. Sometimes lactose intolerance is clinically evident, in most cases it is primary or genetic (hypolactasia adult type) and starts at around 3 to 5 years of age. Lactose intolerance can be a component IBS but it may also complicate several illnesses (secondary lactose intolerance) which result in small intestinal mucosal injury, including Celiac Disease, Crohn’s Disease and bacterial overgrowth. Indeed, hematochezia and other systemic manifestations such as weight loss and fever are not consistent with a diagnosis of primary lactose intolerance.
In conclusion, allergic diseases are increasingly prevalent in our population including children. Specific food hypersensitivity disorders are age-dependent and overlap with functional disorders such as infant colic and recurrent abdominal pain in the older child. Clinicians need to have a clear understanding of the basic pathophysiology in order to effectively diagnose and treat this spectrum of illnesses.
References
- Eigenmann PA. Mechanisms of food allergy. Pediatr Allergy Immunol 2009; 20(1):5-11.
- Sánchez-Valverde F, Gil F, Martinez D et al. The impact of caesarean delivery and type of feeding on cow’s milk allergy in infants and subsequent development of allergic march in childhood. Allergy 2009; 64(6):884-9.
- Thygarajan A, Burks AW. American Academy of Pediatrics recommendations on the effects of early nutritional interventions on the development of atopic disease. Curr Opin Pediatr 2008; 20(6):698-702.
- Exl B-M, Fritsche R. Cow’s milk protein allergy and possible means for its prevention. Nutr 2001; 17:642-51.
- Osborn DA, Sinn J. Soy formula for prevention of allergy and food intolerance in infants. Cochrane Database Systematic Rev (3):CD003741, 2004.
- Agostoni C, Axelsson I, Goulet O et al. Soy protein infant formulae and followon formulae: a commentary by the ESPGHAN Committee on Nutrition. J Pediatr Gastroenterol Nutr 2006; 42:352–61.
- Park MI, Camilleri M. Is there a role of food allergy in irritable bowel syndrome and functional dyspepsia? A systematic review. Neurogastroenterol Motil 2006; 18(8):595-607.
- Elkon KB, Sher R, Seftel HC. Immunological studies of eosinophilic gastro-enteritis and treatment with disodium cromoglycate and beclomethasone dipropionate. S Afr Med J 1977; 12;52(21):838-41.
- Clinical efficacy and pharmacokinetics of montelukast in dyspeptic children with duodenal eosinophilia. Friesen CA, Kearns GL, Andre L et al. J Pediatr Gastroenterol Nutr 2004; 38(3):343-51.
- Melamed I, Feanny SJ, Sherman PM, Roifman CM. Benefit of ketotifen in patients with eosinophilic gastroenteritis. Am J Med 1991; 90(3):310-4.
- Calvani M, Giorgio V, Miceli Sopo S. Specific oral tolerance induction for food. A systematic review. Eur Ann Allergy Clin Immunol 2010; 42(1):11-9.
- Katzka DA. Demographic data and symptoms of eosinophilic esophagitis in adults. Gastrointest Endosc Clin N Am 2008; 18(1):25-32; viii.
Gastrointest Endosc Clin N Am 2008; 18(1):11-23; vii.
- Dellon ES, Farrell TM, Bozymski EM, Shaheen NJ. Diagnosis of eosinophilic esophagitis after fundoplication for ‘refractory reflux’: implications for preoperative evaluation. Dis Esophagus 2010; 23(3):191-5.
- Barada K et al . Celiac disease in Middle Eastern and North African countries: A new burden? World J Gastroenterol 2010; 16(12):1449-57
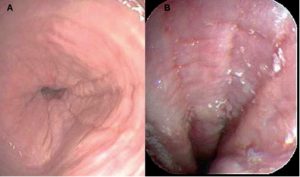
Figure 1 Endoscopic findings in eosinophilic esophagitis. A. Mucosal
rings. B. Longitudinal furrows and nodular mucosa.

{kind=link}