
Imaging the Cervix – Part II
by Pierre Vassallo – This article follows on Part I, which appeared in the last issue of The Synapse Journal. It will discuss imaging of endometriosis in the cervical canal and also cervical cancer. The importance of imaging in staging of cervical cancer will be stressed.
Endometriosis, a benign gynaecologic disorder that affects approximately 10% of women of reproductive age, is defined as endometrial tissue outside the uterus. Cervical involvement with endometriosis is rare occurring in 0.1%–2.4% of patients. Cervical endometriosis may be superficial or deep depending on the depth of penetration of the cervix. The pathogenesis of cervical endometriosis is unknown. Superficial cervical endometriosis may be an incidentally detected histologic finding in asymptomatic women. It may also manifest as a cervical mass, with symptoms of pelvic pain or abnormal vaginal bleeding. On ultrasound, cervical endometriosis may present as a complex cystic mass within the endocervical canal, but may even appear solid extending into the paracervical tissues. In the latter case, it could mimic leiomyomas, polyps, and even carcinoma. Although clinical history and speculum exam may suggest the diagnosis, biopsy confirmation is required.
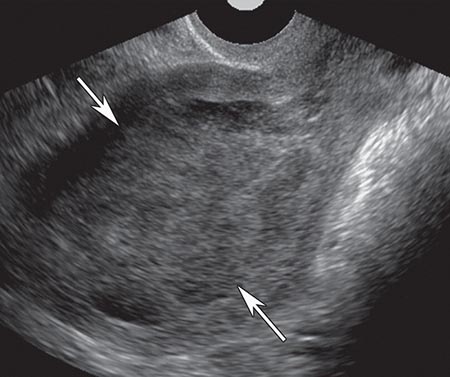
Endometriosis usually presents through symptoms related to peritoneal infiltration, which may be superficial or deep (extending >5mm below the peritoneal surface). Deep infiltrating peritoneal lesions located in the Pouch of Douglas (Fig 1) may penetrate the posterior aspect of the cervix. External cervical penetration from an endometriotic lesion in the Pouch of Douglas would appear as a hypoechoic mass infiltration the posterior cervical stroma on ultrasound, and would mimic peritoneal carcinomatosis or invasive cervical cancer (Fig 2).
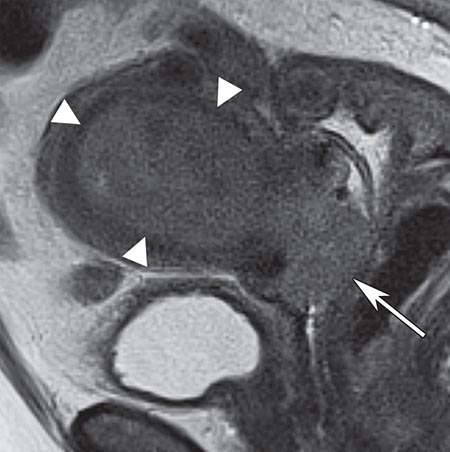
MR imaging may help to establish the correct diagnosis by showing the characteristic low T2 signal intensity resulting from haemosiderin deposition with high T1 signal foci representing fresh haemorrhage (Fig 3).
Cervical cancer is the leading gynecologic cancer worldwide. There are multiple known risk factors for development of cervical cancer, including history of multiple sexual partners, early age of first intercourse, multiparity, lower socioeconomic standing, cigarette smoking, immunosuppressed state, and use of oral contraceptives. There is also a strong association with human papillomavirus (serotypes 16, 18, 31, 33, and 56) accounting for more than 80% of all invasive cervical cancers. The increasing use of the human papillomavirus vaccine appears to be leading to a significant decrease in the incidence of cervical cancer.
The mucosal lining of the cervix is composed of columnar cells in its proximal portion and squamous epithelial cells more distally. The transition zone is the border that separates the proximal columnar lined cervical canal from the distal squamous cell lined portion. The transition zone lies more distally in younger women (20-40 years of age) and moves more proximally with increasing age. The transition zone is the site of development of cervical cancer. Thus cervical cancer tends to be closer to the external os and is more exophytic in younger women, while in older women it lies closer to the internal os and is more endophytic. 80-90% of cervical cancers are squamous cell cancers, while 5-20% (depending on published source) are adenocarcinomas.
Women with cervical cancer tend to present with abnormal vaginal bleeding mainly intermenstrual bleeding (metrorrhagia) and post-menopausal bleeding. Cervical cancer can also lead to cervical canal stenosis and obstruction resulting in hydrometra, haematometra and pyometra.
Accurate staging of cervical cancer is critical for proper management, because risk stratification and mode of treatment depend on tumour size, the presence and extent of local invasion and the presence of metastases. Traditionally, staging of cervical cancer was performed through clinical examination using the FIGO (International Federation of Gynaecology and Obstetrics) staging system (Fig 4). MR imaging provides a more accurate method of the stage of cervical cancer than clinical examination. Thus FIGO staging is now based on MR imaging findings rather than clinical examination. Endovaginal ultrasound is used mainly for detection of cervical cancer.
Tumours restricted to the uterus and upper two thirds of the vagina and <4cm in size (Stage IIa or lower) are amenable to surgery. Tumours >4cm in size, involving the distal third of the vagina or extending to the parametrium, pelvic sidewall, rectum or bladder (Stage IIb and higher) are best treated with radiotherapy and chemotherapy. Tumours <2cm in diameter (Stage 1A2 and 1B1) may be treated with fertility sparing surgery if the remaining cervix is >1cm in length.
Early cervical cancer is difficult to detect on ultrasound due to its small size and similar echotexture to normal cervical mucosa. However, published data has shown that up to 93% of invasive cervical cancer is detected by endovaginal ultrasound. Ultrasound features of cervical cancer include abnormal mucosal echotexture, distortion of cervical morphology and loss of compressibility of the cervix. Cervical cancer also shows increased vascularity on Doppler ultrasound in almost all cases (Fig 5). Occasionally the cervix may be totally replaced by tumour and invasion of adjacent organs may be evident on endovaginal ultrasound (Fig 6). Application of pressure on the endovaginal probe evaluates mobility of the cervix in relation to the rectum, bladder and vagina; lack of mobility indicates adjacent organ involvement.
MR imaging provides accurate evaluation of cervical tumour size and invasion of adjacent structures including the bladder, rectum and parametrial regions (Figs 7-9). Evaluation of the retroperitoneum is required particularly in case of larger tumours to detect lymph node metastases and ureteric infiltration with obstruction; this may be performed with computed tomography (CT) or MR imaging.
Occasionally, a mass in the cervix may be due to inferior extension of an endometrial cancer (Fig 10). This condition may be detected on both endovaginal ultrasound and MR imaging, and its distinction is of clinical relevance as the treatment options for the cervical and endometrial cancer differ.
It is important to note that a number of pitfalls exist in relation to ultrasound assessment of cervical cancer. It is common to see a relative lack of images of the cervix in pelvic ultrasound exams. Failure to visualise and document a normal cervix may lead to missed cervical cancer. An inability to visualise and document a normal cervix may occasionally be the only indicator of disease in the cervix. A mass in a grossly distorted cervix may be erroneously interpreted as a uterine fibroid if a normal cervix has not been properly documented. Hydrometra should also be interpreted with caution as obstruction of the cervical canal may be due to a cervical cancer. In cases where ultrasound does not clearly document a normal cervix, where secondary signs are present (e.g. haematometra) or clinical symptoms are persistent and unexplained, it is prudent to proceed to MR imaging.
Figure Legends

Figure 1. Sagittal endovaginal ultrasound in a case of endometriosis showing moderately echogenic nodule (arrows) with irregular margins lying posterior to the cervix and infiltrating/obliterating the Pouch of Douglas.
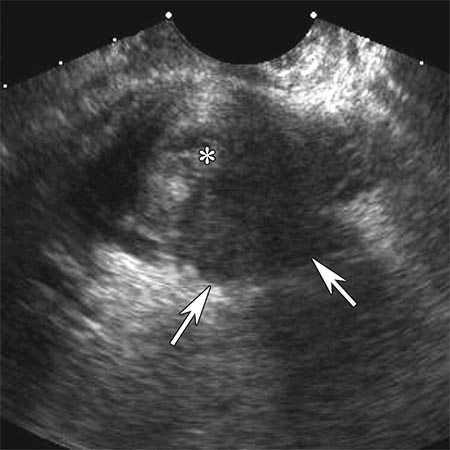
Figure 2. Coronal endovaginal ultrasound scan through the cervix in a case of endometriosis showing a hypoechoic mass centred in the Pouch of Douglas infiltrating the cervix posterolateral to the endocervical canal (*).
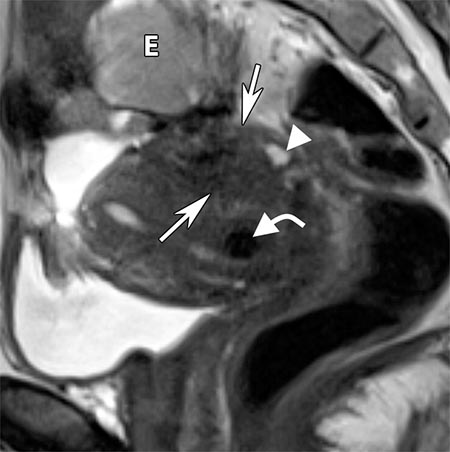
Figure 3. Sagittal T2-w MR image in a case of endometriosis showing an ill-defined mass (arrows) infiltrating the posterior wall of the uterus and cervix and the anterior wall of the rectum. The mass contains hypointense foci (curved arrow) due to haemosiderin content and hyperintense foci (arrowhead) due blood. A hyperintense mass (E) seen superior to the uterus represents an endometrioma.
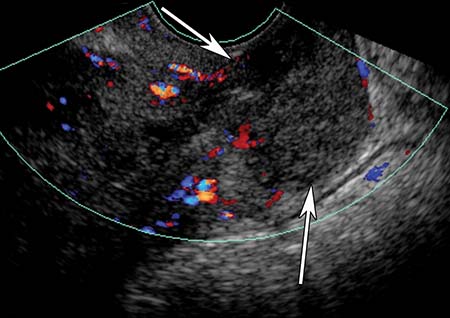
Figure 4. FIGO staging of cervical cancer.
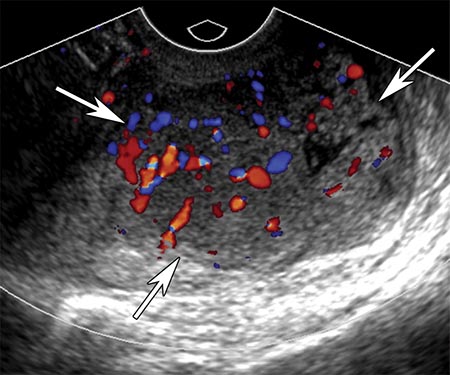
Figure 5. Sagittal endovaginal ultrasound showing a cervical cancer (arrows) that is causing distortion of cervical canal architecture and abnormal echotexture and demonstrates hypervascularity on colour Doppler evaluation.
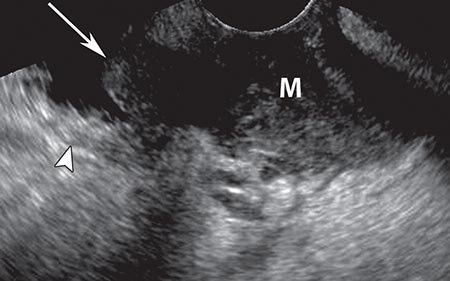
Figure 6. Sagittal endovaginal ultrasound of a locally advanced cervical cancer (M) showing invasion of the bladder wall (arrow). A normal segment of bladder wall (arrowhead) is also seen.
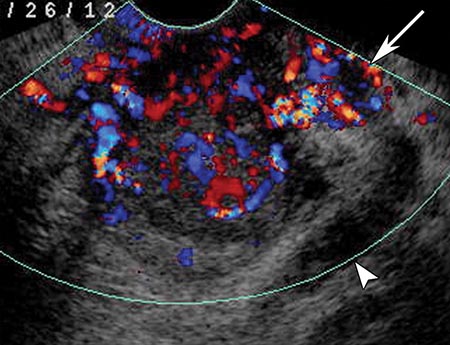
Figure 7. Coronal endovaginal Doppler ultrasound showing a hypervascular tumour with parametrial invasion (arrow) and obstruction of the left ureter (arrowhead).

Figure 8. Sagittal T2-weighted image showing a cervical mass (arrow) of mixed hyperintensity that involves all of the cervical canal and extends into the lower uterus, but does not involve the outer stromal layer, vagina or adjacent organs. A fibroid (*) is incidentally noted.
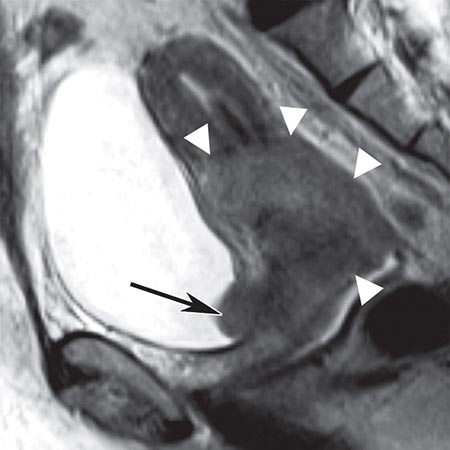
Figure 9. Sagittal T2-weighted image showing an extensive mass (arrowheads) originating from the cervix and involving the uterus and rectum. Extension into the bladder (arrow) is also noted.
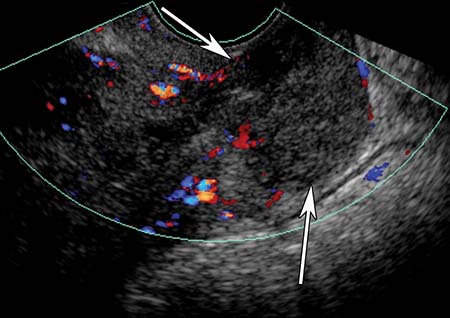
Figure 10a. Sagittal endovaginal ultrasound showing an ill-defined mass in the cervix (arrows).
b. Sagittal endovaginal ultrasound showing a mass in the endometrial cavity of the uterus (arrows).
c. Sagittal T2-weighted MR scan depicting a large mass (arrowheads) extending from the uterine cavity into the cervix and vagina (arrow).