
Imaging Inflammatory Bowel Disease
Pierre Vassallo
Inflammatory bowel disease (IBD) refers to a group of idiopathic conditions of the gastrointestinal tract, the most common of which are Crohn’s disease and ulcerative colitis (UC). Approximately one in every four to six patients with IBD presents in childhood or adolescence. The incidence of IBD has been increasing over the past 40 years.
Crohn’s disease is a chronic inflammatory disease of the gastrointestinal tract that is characterized by waxing and waning symptoms, transmural inflammation of the bowel wall (i.e. all three bowel wall layers), and skip lesions. It may effect any portion of the gastrointestinal tract, in contrast to UC which only effects the colon . UC lesions are also contiguous and do not penetrated beyond the mucosal layer unlike, Crohn’s disease.
IBD can be diagnosed or monitored using a variety of methods, including clinical or hematologic assessment, endoscopy, and imaging. In recent years, an increase in the number of methods used to visualize the bowel has become available, including capsule endoscopy, CT enterography, and MR enterography, with each study having its advantages and disadvantages.
CT or MR enterography is tailored to evaluate the small bowel and its mucosa. Both studies provide exquisite detail of the bowel wall, including its thickness and mucosa, while also allowing detection of the extraenteric manifestations and complications of IBD.
Both CT and MR enterography provide high quality small bowel imaging. CT enterography has the advantages of better spatial resolution, fewer motion artifacts, lower cost, shorter examination times and increased tolerance by claustrophobic patients. On the other hand, MR enterography has the advantage of not using ionizing radiation; this is therefore preferable in children and in pregnant women. MR enterography offers also higher contrast resolution and better evaluation of perianal disease, while also allowing assessment of peristalsis through dynamic imaging.
When comparing CT or MR enterography to traditional small bowel barium follow-through exam, the former are more accurate in detecting IBD, while CT enterography performed on new generation scanners that use iterative reconstruction technologies, exposes the patient to a smaller radiation dose than a small bowel barium exam.
Small bowel endoscopy rarely covers the whole small bowel and therefore misses a significant number of cases with small bowel inflammatory disease. Capsule endoscopy is performed with an 11 x 27mm capsule that is swallowed by the patient and that records images as it passes through the gastrointestinal tract. It is superior to all other tests for detecting mucosal changes, however it is unable to detect transmural extent of disease and extraenteric manifestations. The capsule is difficult to swallow particularly in children. In addition, due to the frequent presence of bowel strictures particularly in Crohn’s disease, there is a high risk of capsule retention (8%), which would consequently require open surgery further increasing the risk of complicating structures, fistulae and abscess formation. Thus a barium study is required prior to capsule endoscopy in order to exclude strictures and minimize the risk of capsule retention.
The technique for performing CT or MR enterography is quite complex and is beyond the scope of this article. The imaging findings are similar on both CT and MR imaging; they can be divided into (1) intestinal and (2) extra-intestinal findings.
1. Intestinal findings
The intestinal findings include bowel wall thickening (bowel wall thickness >3mm in a distended loop), mucosal enhancement, mural layering, skip lesions, luminal narrowing/strictures and fistula. Bowel wall thickening (Fig 1) is the most common finding in IBD particularly in Crohn’s disease. Mucosal enhancement is the strongest indicator of acute inflammation and is often accompanied by mural stratification (Fig 2). Bowel wall thickening is also clearly evident on MR enterography (Fig 3) as is mucosal enhancment (Fig 4). Mural stratification may also be the result of fat deposition in between the mucosa and serosa; this occurs in chronic IBD and can be confirmed with fat suppression techniques on MR enterography. Skip lesions are discontinuous areas of inflammation in either the small bowel or colon and are characterized by either mucosal enhancement or bowel wall thickening; these are pathognomonic of Crohn’s disease (Fig 4).
Diffusion-weighted imaging (DWI) is a special technique that is available on MR imaging, which measures the diffusivity of extracellular water. Acutely inflammed bowel has an excess of extracellular fluid that naturally has a high diffusivity; this is well seen on DWI and can be used to identify active bowel wall inflammation (Fig 5).
Luminal narrowing and strictures may be identified either through actual narrowing of the luminal diameter (Fig 6) or indirectly through dilatation of the more proximal bowel loops (Fig 7).
Patients with Crohn’s disease have a 20–40% lifetime risk of fistula formation and the most common fistulas are enterocutaneous, enteroenteric, and perianal fistulas (Fig 8).
2. Extra-intestinal findings
The extra-intestinal findings include engorgement of mesenteric vessels (comb sign), mesenteric infiltration, increased mesenteric fat, lymphadenpathy, fluid collections (abscess formation) and ascites. Engorgement of the vasa recta is a finding of active inflammation in IBD and is caused by increased blood flow through the vasa recta to inflamed segments of bowel; this may result in the comb sign (Fig 9). Extension of inflammation outside the bowel wall results in mesenteric infiltration that appears as fat stranding on MR and CT enterography (Fig 10). An increase in number and size of mesenteric lymph nodes (frequently only mildly enlarged) is seen in IBD (Fig 11).
Other non-bowel related features, which include gall stones, nephrolithiasis, primary sclerosing cholangiitis, sacroiliitis and thromboembolism are all detected on images obtained during CT and MR enterography.
CT and MR enterography are safe and effective methods for diagnosing and evaluating IBD; unlike previous x-ray contrast techniques and endoscopy, these methods allow radiologists to interpret intestinal and extra-intestinal findings that are widespread and which are of great importance in these patients.
Figure Legends

Figure 1. Coronal CT enterographic image showing multiple areas of bowel wall thickening throughout the abdomen (arrows) in this patient with Crohn’s disease.
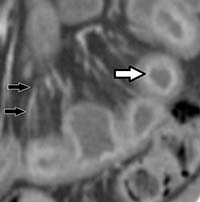
Figure 2. Coronal CT enterographic image showing mucosal enhancement and mural stratification (white arrow) as well as engorged mesenteric blood vessels (vasa recta) (black arrows) in this patient with Crohn’s disease.
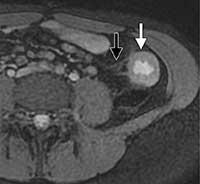
Figure 3. MR enterographic image shows bowel wall thickening of the descending colon (white arrow) and wispy increased signal intensity in the surrounding pericolonic fat (black arrow).

Figure 4. Coronal post-IV contrast T1-weighted MR enterographic image showing discontinuous regions of bowel wall thickening and mucosal enhancement (arrows).

Figure 5. Coronal diffusion-weighted image with background body shows an S-shaped area of restricted diffusion corresponding to the terminal ileum (arrows).
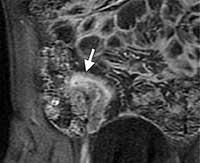
Figure 6. Coronal CT enterographic image showing narrowing of the lumen of the terminal ileum (white arrow) in Crohn’s disease.

Figure 8. Axial T1-weighted MR entrograph shows a fistula between the colon and uterus (white arrow), a short-segment stricture (arrowhead) just proximal to the fistula and more proximal small bowel dilatation (black arrow).

Figure 9. Oblique coronal CT enterographic image shows abnormal bowel wall thickening, mucosal hyperenhancement of the terminal ileum and engorgment of the vasa recta (arrows) creating the comb sign.

Figure 10. Fat stranding within the pericecal fat (arrows) seen on axial CT enterography.
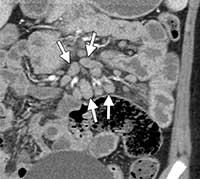
Figure 11. Prominent mesenteric lymph nodes (increase in size and number of lymph nodes) (arrows) seen on coronal CT enterography.