Imaging Coeliac Disease
Pierre Vassallo
Coeliac disease is one of the most common chronic health disorders in western countries. It is also one of the most under-diagnosed. Up until ten years ago, medical schools taught that coeliac disease was relatively rare and only affected about 1 in 2,500 people. It was also thought to be a disease that primarily affected children and young people. Recent studies and advances in diagnosis show that at least 1 in 133 people have coeliac disease, but only 1 in 4,700 is ever diagnosed.
While in the past diarrhoea was considered to be the main feature of coeliac disease, we now know that constipation is almost as common and many individuals have no alteration in bowel habit. Weight loss was also claimed to be a salient symptom of coeliac disease. We now know that only 5% of patients with the disease are underweight, while 39% are overweight and 13% are obese.
The main symptoms of coeliac disease are abdominal pain, irondeficiency anaemia and a positive faecal occult blood test. At a later stage, lactose intolerance, osteoporosis, increased fracture risk, miscarriage, low birth weight, lymphoma, seizures, and depression may occur.
Coeliac disease is a chronic autoimmune disorder induced in genetically susceptible individuals after ingestion of gluten proteins, which are found in wheat, rye, barley, and certain other grains.
The small bowel mucosa is primarily affected, resulting in progressive degrees of villous inflammation and destruction with resulting induction of crypt hyperplasia. The destruction begins in the duodenum and over time progresses distally to the ileum. Loss of villi, which absorb fluid, and hypertrophy of crypts, which produce fluid, result in chronic fluid excess in the small bowel lumen.
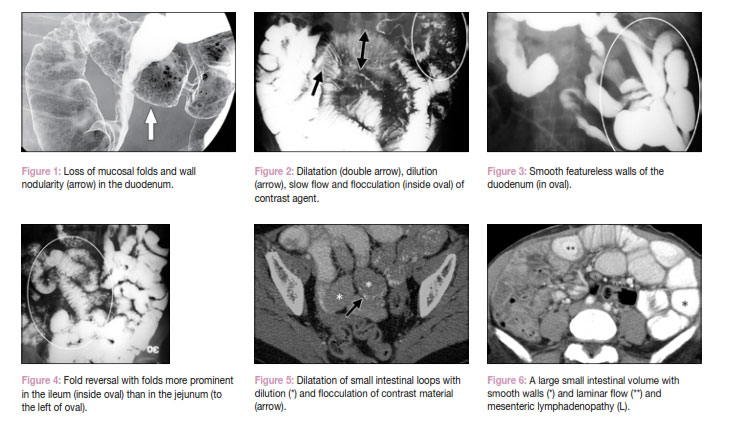
Access intraluminal fluid and its effects of small bowel wall structure were described around three decades ago on small bowel barium sulphate studies. These include (1) loss of mucosal folds and wall nodularity in the duodenum (Figure 1), (2) dilatation, dilution, slow flow and flocculation of contrast agent (Figure 2), (3) smooth featureless walls of the duodenum due to villous atrophy and wall oedema (Figure 3) and (4) fold reversal, whereby folds are more prominent in the ilieum than in the jejunum (Figure 4). The number of double contrast small bowel barium examinations performed and the skill necessary to interpret their results are both in decline as the technique is both time-consuming and also very uncomfortable for the patient. A small bowel barium study (also called small bowel enteroclysis) requires trans-nasal insertion of a tube into the duodenum followed by pump administration of barium sulphate followed by about 2 litres lactulose solution.
Antibody testing for coeliac disease is both sensitive and also highly specific; it involves testing for anti-tissue transglutaminase and anti-endomysial antibodies. However, antibody tests and also barium small intestinal studies are unlikely to be performed if there is no clinical suspicion for coeliac disease.
Abdominal pain in coeliac disease is a common early complaint that often leads to computed tomography (CT). Thus CT may the first study available that can suggest the diagnosis of coeliac disease as well as showing the severity of the condition.
CT findings in coeliac disease include all the malabsorptive patterns described above for small bowel barium studies as well as mesenteric lymphadenopathy and large bowel findings both of which are not detectible with small bowel contrast radiography. Therefore CT is likely to be more sensitive in detecting coeliac disease than barium studies.
Malabsorptive features on CT include dilatation of small intestinal loops with dilution and flocculation of contrast material (Figure 5) and a large small intestinal volume with smooth walls and laminar flow and mesenteric lymphadenopathy (Figure 6). Laminar flow occurs due to wide intestinal caliber and may mimic intusussecption. Intusussception is also more likely to occur in coeliac disease.
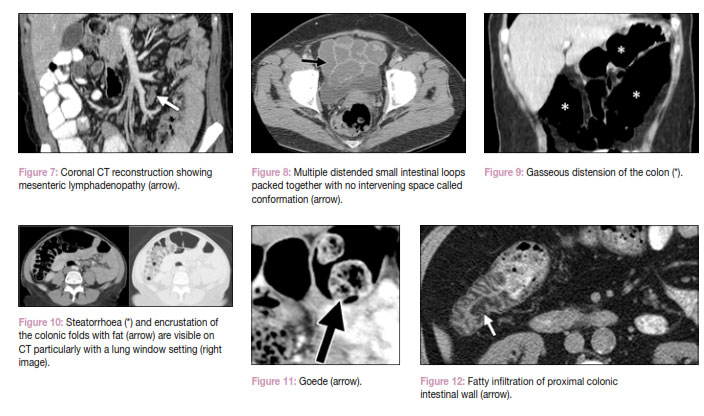
Chronic lymphatic stimulation with follicular hypertrophy and an increase in T and B lymphocytes is responsible for mesenteric lymphadenopathy (Figure 7) and is also thought to be the cause of the elevated lymphoma risk in coeliac disease.
Conformation is a term used to describe multiple distended small intestinal loops packed together with no intervening space; this is also suggestive of coeliac disease (Figure 8)
On reaching the colon, sugar and fat that are undigested by the small bowel will be “digested” by gasproducing bacteria, altering colonic function and structure. Chronic excess gas production will distend the colon, decreasing its tone and altering the appearance of both the colon and stool (Figure 9). Steatorrhoea and encrustation of the colonic folds with fat are visible on CT particularly with a lung window setting (Figure 10). Ball shaped stools containing air and fat in the centers may also be seen, these are known as “geodes” (Figure 11). Normally, there should be very little fluid in the colon; abundant colonic fluid seen on CT may be seen in coeliac disease. Fatty infiltration of small intestinal and colonic wall (Figure 12) and splenic atrophy are also features of coeliac disease.
Colonic CT features alone are not specific for coeliac disease, however when combined with small intestinal findings and lymphadenopathy, they are strongly suggestive of the disease. CT is proving increasingly useful for the detection of a wide variety of intestinal diseases. It has the advantage of also evaluating all abdominal solid organs that may alter investigative algorithms to reach a correct diagnosis more rapidly. This in turn, reduces morbidity and mortality. The recently recognized high prevalence of coeliac disease makes it likely that some “healthy” subjects in past studies may have had coeliac disease. Patients with chronic abdominal pain particularly those classified as IBS (irritable bowel syndrome) may benefit from clinical and radiological review as coeliac disease is a much more treatable condition.
Important Note: The article does not discuss invasive tests that are sometimes used to confirm coeliac disease. These include gastroduodenoscopy, jejunoscopy (with biopsy) and video capsule endoscopy. These techniques have a relatively high false negative rate and are technically difficult to perform. CT is a non-invasive procedure that may suggest coeliac disease when investigating abdominal pain, even when the diagnosis was not initially considered. Combining CT findings with antibody testing would avoid unnecessary invasive procedures.