
How Big is the Diabetes Type 2 Problem?
Author : Prof. Albert Cilia-Vincenti
The US Centers for Disease Control and Prevention recently claimed that more than 1 in 3 American adults have blood sugar levels that are too high.1 They included prediabetics in their statement.
In 2016, the University of California, Los Angeles (UCLA), reported that 55% of Californian adults are either prediabetic or have undiagnosed type 2 diabetes (Figure 1).2 Prediabetes is not a nit-picking philosophical concept. Diabetic pathologies develop during prediabetes3 and, by the time type 2 diabetes manifests itself, patients may already have kidney impairment,4,5 vision loss,6-8 neuropathy,9 atherosclerosis10-12 and cancer.13-15 Excessive food and drink intake, particularly the high glycaemic ones, spike blood sugar levels which also accelerate ageing by shortening telomeres.16,17
The goalposts for safe blood glucose levels have been changing. Levels considered dangerous now were thought to be safe decades ago. Current recommendation is for blood sugar to be kept at the low end of the normal reference range.18-21 However, a significant section of the medical community may have failed to wake up to the life-shortening impact of prediabetes.
One diagnostic problem is that prediabetes and early stage diabetes may be missed by the standard fasting blood glucose in the presence of hyperinsulinaemia. As long as there is reasonable insulin sensitivity and hyperinsulinaemia, a fasting blood glucose may appear to be in a safe range, which is conventionally considered to be under 5.6 mmol/L, although some claim the safe upper limit ought to be 4.7mmol/L.
Hyperinsulinaemia contributes to disease states (e.g. hypertension, blood hypercoagulability and increased cancer risk) even before fasting blood glucose rises to what conventional medicine regards as prediabetic levels, namely, 5.6 – 6.9 mmol/L. For the above reasons, and in this scenario, the fasting blood glucose test should perhaps now be considered dangerously obsolete.
The haemoglobin A1c (HbA1c) blood test provides a better picture of glycaemic control than fasting blood glucose,22 but is probably underutilised in identifying prediabetes. The safe upper limit for HbA1c is considered 5.5%, but lower ranges have been shown to be healthier.23 HbA1c between 5.6% and 6.4% is diagnostic for prediabetes.24
Metformin ought to be prescribed when the HbA1c is between 5.6% and 6.4% for prevention of type 2 diabetes,25 together with advice on calorie restriction and, in particular, the high glycaemic ones. Metformin enhances insulin sensitivity and functions via several mechanisms to improve glycaemic control.26-30 It has proven ability to delay or prevent type 2 diabetes.31-33 Yet recent US surveys reveal it is prescribed to only 3.7% to 8.1% of prediabetics.33-35
Perhaps the term prediabetes is a misnomer because even modestly elevated glucose levels inflict microvascular damage resembling the long-term complications of type 2 diabetes.36,37 Excess glucose is converted to triglycerides that are stored as fat (subcutaneous and abdominal) and which may result in fatty liver disease (may progress to cirrhosis and hepatocellular carcinoma). Excess glucose is inflammatory to many tissues, including arteries (atherosclerosis).38-40 High “normal” blood sugar levels are increasingly recognised as posing an increased risk of degenerative disorders.4-15,20,41-49
Fasting blood glucose values in the upper “normal” range (above 4.7mmol/L) appear to be an important independent predictor of cardiovascular death in nondiabetic, apparently healthy, middle-aged men.18 After-meal glucose levels are an even stronger predictor of disease risk.50-52
About 70% of prediabetics will develop type 2 diabetes in their lifetime.53,54 It is misleading to think that prediabetes relates to a period where no diabetic damage is caused. Coronary heart disease risk is similar between prediabetics and type 2 diabetics.47
Early detection of prediabetes means a greater likelihood of reversing it before it progresses to type 2 diabetes. Glucose-lowering approaches should be initiated when HbA1c exceeds 5.5% and not delayed till it reaches 6.5%.
In the area of laboratory predictive testing for cardiovascular risk, we have probably underestimated the importance of the prediabetic state (as defined by HbA1c levels above). For around 60 years we accepted the hype around cholesterol, dietary saturated fats, heart attacks and now, statins. In spite of the huge global expense on cholesterol testing and statins, atherosclerotic-related morbidity and mortality remains number one in industrialised countries.
The clinical significance of the various blood lipoproteins is still confused. We now know that there are at least two main types of LDL cholesterol, a small, dense atherogenic particle and a larger lighter one thought to be harmless. The different LDL particles are too expensive to be measured routinely. We therefore don’t know whether a high LDL is due to an elevated “harmless” or “bad” LDL sub-fraction. Adding “non-HDL cholesterol” to routine testing is even more confusing. The combination of a raised fasting triglycerides level and a low HDL level is a surrogate marker for raised “bad” LDL (see previous features in the The Synapse Medical Journal on the Cholesterol Controversy). What raises fasting triglycerides levels and lowers HDL are high glycaemic carbohydrates and alcohol, rather than saturated fats.
Glucose may be a more important damaging inflammatory agent than saturated fats. The French have the lowest heart disease mortality in Europe (and second lowest worldwide). Malta has almost three times the heart disease mortality of France. The reason is not Maltese consumption of dairy produce and meats being three times that in France. Obesity and blood glucose levels might be the main problem, rather than cholesterol. Perhaps about half our adult population is prediabetic or already diabetic, like California. Who knows?
The term “prediabetes” may render a false sense of normality. Perhaps the progression stages of type 2 diabetes could more realistically be renamed, “early diabetes”, “established diabetes” and “end-stage (insulin-dependent) diabetes”. A false sense of normality is also fostered by laboratories in Malta stating a “normal range” for HbA1c of up to 6.5%, when it should be up to 5.5%.
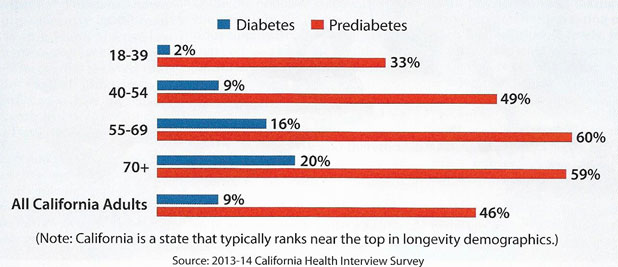
Figure 1: Diabetes cases by age group. A UCLA study found that 55% of adults in California have either diabetes or prediabetes.2
References
- https//www.cdc.gov/features/diabetesfactsheet/.
- Babey SH, Wolstein J, Diamant AL et al. Prediabetes in California: Nearly Half of California Adults on Path to Diabetes. Policy Brief UCLA Cent Health Policy Res. 2016 (Pb2016-1): 1-8.
- Tabak AG, Herder C, Rathmann W et al. Prediabetes: a high-risk state for diabetes development. Lancet 2012; 379 (9833): 2279-90.
- Plantinga LC, Crews DC, Coresh J et al. Prevalence of chronic kidney disease in US adults with undiagnosed diabetes or prediabetes. Clin J Am Soc Nephrol. 2010; 5 (4): 673-82.
- Hoehner CM, Greenlund KJ, Rith-Najarian S et al. Association of the insulin resistance syndrome and microalbuminuria among nondiabetic native Americans. The Inter-Tribal Heart Project. J Am Soc Nephrol. 2002; 13(6): 1626-34.
- Gabir MM, Hanson RL, Dabelea D et al. Plasma glucose and prediction of microvascular disease and mortality: evaluation of 1997 American Diabetes Association and 1999 World Health Organisation criteria for diagnosis of diabetes. Diabetes Care 2000; 23 (8): 1113-8.
- Algvere P, Elendic S, Luft R et al. Retinal microangiography and pigment epithelial lesions in subjects with normal, borderline, and decreased oral glucose tolerance. Br J Ophthalmol. 1985; 69 (6): 416-9.
- Tapp RJ, Tikellis G, Wong TY et al. Longitudinal association of glucose metabolism with retinopathy: results from the Australian Diabetes Obesity and Lifestyle (AusDiab) study. Diabetes Care 2008; 31 (7): 1349-54.
- Sumner CJ, Sheth S, Griffin JW et al. The spectrum of neuropathy in diabetes and impaired glucose tolerance. Neurology 2003; 60 (1): 108-11.
- Redgrave JN, Lovett JK, Syed AB et al. Histological features of symptomatic carotid plaques in patients with impaired glucose tolerance and diabetes (oxford plaque study): Cerbrovasc Dis. 2008; 26(1): 79-86.
- Kurihara O, Takano M, Yamamoto M et al. Impact of prediabetic status on coronary arthersclerosis: a multivessel angioscopic study. Diabetes Care 2013; 36(3): 729-33.
- Kramer D, Raji A, Plutzky J. Prediabetes mellitus and its links to atherosclerosis. Curr Diab Rep. 2003; 3 (1): 11-8.
- Huang Y, Cai X, Qiu M. et al. Prediabetes and the risk of cancer: a meta-analysis. Diabetologia. 2014; 57 (11): 2261-9.
- Salinas-Martinez AM, Flores-Cortes LI, Cardona-Chavarria JM et al. Prediabetes, diabetes and risk of breast cancer: a case-control study. Arch Med Res. 2014; 45 (5): 432-8.
- Onitilo AA, Stankowski RV, Berg RL et al. Breast cancer incidence before and after diagnosis of type 2 diabetes mellitus in women: increased risk in the prediabetes phase. Eur J Cancer Prev. 2014; 23 (2): 76-83.
- Leung CW, Laraia BA, Needham BL et al. Soda and cell aging: associations between sugar-sweetened beverage consumption and leukocyte telomere length in healthy adults from the national health and Nutrition Examination Surveys. Am J Public Health 2014; 104 (12): 2425-31.
- Adaikalakoteswari A, Balasubrmanyam M, Ravikumar R et al. Association of telomere shortening with impaired glucose tolerance and diabetic macroangiopathy. Atherosclerosis 2007; 195 (1): 83-9.
- Bjornholt JV, Erikssen G, aaser E et al. Fasting blood glucose: an underestimated risk factor for cardiovascular death. Results from a 22-year follow-up of healthy nondiabetic men. Diabetes Care 1999; 22 (1): 45-9.
- Selvin E, Coresh J, Golden SH et al. Glycemic control and coronary heart disease risk in persons with and without diabetes: the atherosclerosis risk in communities study. Arch Intern Med 2005; 165 (16): 1910-6.
- Levitan EB, Song Y, Ford ES et al. Is nondiabetic hyperglycemia a risk factor for cardiovascular disease? A meta-analysis of prospective studies. Atch Intern Med 2004; 164 (19): 2147-55.
- Held C, Gerstein HC, Yusul S et al. Glucose levels predict hospilisation for congestive heart failure in patients at high cardiovascular risk. Circulation 2007; 115 (11): 1371-5.
- Selvin E, Steffes MW, Zhu H et al. Glycated haemoglobin, diabetes and cardiovascular risk in nondiabetic adults. N Engl J Med 2010; 362 (9): 800-11.
- Matsushita K, Blecker S, Pazin-Filho A et al. The association of haemoglobin A1c with incident heart failure among people without diabetes: the atherosclerosis risk in communities study. Diabetes 2010; 59 (8): 2020-6.
- Prediabetes, WebMD, 2018.
- Standards of Medical Care in Diabetes – 2014. Daibetes Care 2014; 37 (supplement 1): S14-S80.
- Giannarelli R, Aragona M, Coppelli A et al. Reducing insulin resistance with metformin: the evidence today. Diabetes Metab 2003; 29 (4 Pt 2): 6s28-35.
- Malin SK, Gerber R, Chipkin SR et al. Independent and combined effects of exercise training and metformin on insulin sensitivity in individuals with prediabetes. Diabetes Care 2012; 35 (1): 131-6.
- Hundal RS, Krssak M, Dufour S et al. Mechanism by which metformin reduces glucose production in type 2 diabetes. Diabetes 2000; 49 (12): 2063-9.
- Caton PW, Nayuni NK, KiewishJ et al. Metformin suppresses hepatic gluconeogenesis through induction of SIRT1 and GCNS. J Endocrinol 2010; 205 (1): 97-106.
- Hostalek U, Gwilt M, Hildermann S. Therapeutic Use of Metformin in Prediabetes and Diabetes Prevention. Drugs 2015; 75 (10): 1071-94.
- Lily M, Godwin M. Treating prediabetes with metformin: systematic review and meta-analysis. Can Fam Physician. 2009; 55 (4): 363-9.
- Salpeter SR, Buckley NS, Kahn JA et al. Meta-analysis: metformin treatment in persons at risk for diabetes mellitus. Am J Med 2008; 12 (2): 149-57.e2.
- Moin T, Li J, Duru OK et al. Metformin prescription for insured adults with prediabetes from 2010 to 2012: a retrospective cohort study. Ann Intern Med 2015; 162 (8): 542-8.
- Sterling DL, Onor I, Sarpong D et al. Prescribing Patterns of Metformin in High-risk Patients with Prediabetes. J La Stae Med Soc 2015; 167 (6): 257-62.
- Goldberg T, Kroehl ME, Suddarth KH et al. Variations in Metformin Prescribing for Type 2 Diabetes. J Am Board Fam Med 2015; 28 (6): 777-84.
- Milman S, Crandall JP. Mechanisms of vascular complications in prediabetes. Med Clin North Am 2011; 95 (2): 309-25, vii.
- Sprague RS, Ellsworth ML. Vascular disease in prediabetes: new insights derived from systems biology. Mo Med 2010; 107 (4): 265-9.
- Ebenbichler CF, Kirchmair R, Egger C et al. Postprandial state and atherosclerosis. Curr Opin Lipidol 1995; 6 (5): 286-90.
- Jacobson TA, Miller M, Schaefer EJ. Hypertriglyceridemia and cardiovascular risk reduction. Clin Ther 2007; 29 (5): 763-77.
- Welin I, Erikson H, Larsson B et al. Triglycerides, a major coronary risk factor in elderly men. A study of men born in 1913. Eur Heart J 1991; 121 (6): 700-4.
- Stattin P, Bjor O, Ferrari P et al. Prospective study of hyperglycemia and cancer risk. Diabetes Care 2007; 30 (3): 561-7.
- Muti P, Quattrin T, Grant BJ et al. Fasting glucose is a risk factor for breast cancer: a prospective study. Cancer Epidemiol Biomarkers Prev 2002; 11 (11): 1361-8.
- Cust AE, Kaaks R, Friedenreich C et al. Metabolic syndrome, plasma lipid, lipoprotein and glucose levels, and endometrial cancer risk in the European Prospective Investigation into Cancer and Nutrition (EPIC). Endocr Relat Cancer 207; 14 (3): 755-67.
- Schoen RE, Tangen CM, Kuller LH et al. Increased blood glucose and insulin, body size, and incident colorectal cancer. J Natl Cancer Inst 1999; 91 (13): 1147-54.
- Couthinho M, Gerstein HC, Wang Y et al. The relationship between glucose and incident cardiovascular events. A metaregression analysis of published data from 20 studies of 95,783 indiciduals followed for 12.4 years. Diabetes Care 1999; 22 (2): 233-40.
- Lambin N, Cuvelier E, Gonon X et al. Abstract 2372: Hemoglobin A1c Levls are Associated with Severity and Prognosis of Systolic Chronic Heart Failure in Non Diabetic Patients. Circulation 2006; 114 (Suppl 18): II_486-II_7.
- Li Q, Chen AH, Song XD et al. Analysis of glucose levels and the risk for coronary heart disease in elderly patients in Guangzhou Haizhu district. Nan Fung Yi Ke Da Xue Xue Bao 2010; 30 (6): 1275-8.
- Pereg D, Elis A, Neuman Y et al. Cardiovascular risk in patients with fasting blood glucose levels within normal range Am J Cardiol 2010; 106 (11): 1602-5.
- Bitra YR, Rapaka D Akula A. Prediabetes and Alzheimer’s Disease. Indian J Pharm Sci 2015; 77 (5): 511-4.
- Moebus S, Gores L, Losch Cet al. Impact of time since last calories intake on blood glucose levels. Eur J Epidemiol 2011; 26 (9): 719-28.
- Onat A, Can G, CicekG et al. Fasting, on-fasting glucose and HDL dysfunction in risk of pre-diabetes, diabetes, and coronary disease in non-diabetic adults. Acta Diabetol 2013; 50 (4): 519-28.
- Sacks DB. A1c versus glucose testing: a comparison. Diabetes Care 2011; 34 (2): 518-23.
- Nathan DM, Davidson MB, DeFronzo RA et al. Impaired fasting glucose and impaired glucose tolerance: implications for care. Daibetes Care 2007; 30 (3): 753-9.
- Eikenberg JD, Davy BM. Prediabetes: a prevelant and treatable, but often unrecognized, clinical condition. J Acad Nutr Diet 2013: 113 (2): 213-8.