
Failing to prepare is preparing to fail
Michael Spiteri
By their very nature, mass casualty events are difficult to predict; therefore the nature, location and time of incidents, as well as their impacts are almost unclear to the disaster planners. The ability of an emergency medical system to deal with acute, unexpected increases in medical demands during disasters is a concept endorsed by the vast majority of emergency planners.
Although enjoying stability and relatively free from severe adverse natural phenomena, Malta still had its fair share of mass casualty events. Most of the major mass events were restricted to times of war and unrest in the rest of the world. As a result, our Island is dotted with the remains of grand historical buildings that served as hospitals and medical camps in the past. However, coming closer to our times, we have also witnessed incidents which although not on such a large scale, still tested our resilience and capacity.
Over the past years there have been numerous attempts to determine which method is best suited to ensure that the level of preparedness of a health system caters for the requirements on the day of an incident. Resource management is an element of disaster preparedness, where surge capacity is defined as the maximum potential delivery of required resources, either through augmentation or modification of resource allocation. At the hospital setting, it is the ability to increase available resources in order to cope with an unplanned sudden increase in patients, which is based on a qualitative and quantitative conceptual framework on the basis of four main pillars; stuff, staff, space and systems, better known as the 4S system. Surge capacity and capability come at a cost and it is a fact that no one, either the government or a private medical sector, can afford to pay for unused capacity. Therefore, emergency planners are responsible for achieving the best balance between cost and requirements to maintain the required capacity and capability of a hospital for disasters.
It is a fact that the level of medical care in Malta rose exponentially over the past and today it is regarded amongst the top players in Europe. However, for the reasons mentioned above, our surge capacity and resilience did not enjoy the same growth. On the contrary, the total number of available acute medical beds in Malta over the past thirty years is now probably at its lowest since the Second World War. It is historically documented that up to May 1917 the total number of hospital beds in Malta was just short of 27,000.1 Ever since, the decline in the number of hospital beds is of course fully justifiable given the fact that there was certainly no financial justification to account for the continued upkeeping of hospitals and other health care facilities when the acute demand was not as high.
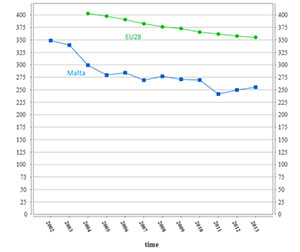
A recent study2 focusing on the surge capacity of Mater Dei Hospital indicated that, although it provides an excellent medical service on a day-to-day basis, it might face significant challenges in the event of a mass casualty event. The root of this difficulty to surge to meet the demands of even a modest mass casualty event is multi-factorial and complex. One of the main reasons for this limitation lies within the fact that unlike other bigger countries, Malta has only one major hospital which is responsible to deliver the care to a whole nation. This responsibility will still need to be carried during a mass casualty event. Although, some smaller hospitals do exist in Malta, our country is probably almost unique, since in the vast majority, private hospitals utilise the medical services of professionals who are also included within the public sector. Therefore, it is anticipated that during such events, private hospitals might actually have a difficulty in providing extra services. This study also concluded that the overall training of medical staff in major incident and mass casualty preparedness is still very low. As a result it is expected that during such events, medical professionals will try to provide the same level of medical care that is provided on a day-to-day basis which will result in the creation of significant critical bottlenecks within the system. Another challenge which has been highlighted within our health care system is space. This phenomenon is similarly witnessed in other health care systems around the world, and as described above it transcends from the value for money mindset which does not allow for any unused bed capacity. Figure 1 clearly shows that in the vast majority, countries across the European Union actually witnessed a decrease in their curative hospital bed capacity over the past years.
Figure 1. Number of curative beds per 100,000 inhabitants across the EU and Malta
|
Number of curative beds per 100,000 inhabitants |
 |
As health care professionals, we have been entrusted with the responsibility of ensuring the best possible care of our patients. This responsibility will also need to be extended during exceptional and unexpected ciscumstances. In view of this commitment, our medical community should look beyond our day-to-day operations and should start considering and formulating plans to improve on our surge capacity. This might sound counterintuative when such requirments are superimposed on our day-to-day challenges to cope with routine load; however it is during these periods of heavy workload that the need for surge increases. Although the space and structural capacity need significant investment and are considered as medium to long-term investments, the concept of including major incident training in acute speciality training should be considered. This new approach has been adopted in the local national Emergency Medicine specialist training curriculum and it is aimed to better prepare our frontliners to provide emergency medical care under non-routine circumstances. It is through these initiatives that we take our level of preparedness to the next level. Not being prepared is not an option; it is just a recipie for failure.
| The research work disclosed in this publication is partially funded by the Strategic Educational Pathways Scholarship (Malta). This Scholarship is part-financed by the European Union – European Social Fund (ESF) under Operational Programme II – Cohesion Policy 2007-2013, “Empowering People for More Jobs and a Better Quality Of Life”. |
References
1. Macpherson WG. History of the Great War. Medical Services. General History. Volume I. London;1921.
2. Spiteri M. Modelling of hospital surge capacity for a mass casualty event respnse in a small island state hospital. European Masters in Disaster Medicine. Thesis 2014.