
Epidemiology of Cardiovascular mortality in the Maltese Islands
Kathleen England
Abstract
Cardiovascular diseases which comprise cardiac causes (most commonly ischemic heart disease and heart failure), cerebrovascular disease and other vascular conditions are the leading cause of death in Europe and worldwide. Despite a downward trend in cardiovascular mortality in many European countries, large disparities exist. Locally, cardiovascular mortality accounted for 40% of all deaths or 1298 deaths in 2013.
Introduction
Global deaths from cardiovascular disease (CVD) are increasing as a result of population growth, the ageing of populations, and epidemiologic changes in disease.1 The World Health Organisation estimated that 31% of all deaths worldwide (17.5 million deaths) were caused by CVD in 2012,2 more than all communicable, maternal, neonatal and nutritional disorders combined, and double the number of deaths caused by cancers.3
Global deaths from CVD increased by 41% between 1990 and 2013 despite a 39% decrease in age-specific death rates; this increase was driven by a 55% increase in mortality due to the aging of the populations and a 25% increase due to population growth. The relative contribution of these drivers varied by region; only Central and Western Europe had gains in cardiovascular health that were sufficient to offset these demographic forces.1
CVD is the leading cause of death in Europe, with 51% of women and 42% of men dying from this disease (40 of the 52 countries provided data up to 2012). The gender difference in the proportional contribution of CVD is driven far more by stroke and other CVD rather than coronary heart disease. Three in every ten deaths of Europeans aged < 65 years and 37% of all deaths occurring < 75 years are attributable to CVD.4
However, there are wide variations between countries in Europe. Some countries have identified cancer as being the commonest cause of death in men (e.g. Belgium, Denmark, France, Luxembourg, Netherlands, Portugal, Spain, Slovenia and San Marino) and for the first time, cancer has surpassed CVD as a cause of death among women in Denmark. In other countries (21 European countries) CVD deaths are more than double the cancer deaths in men and in another 6 countries, male CVD deaths are more than four times greater than cancer deaths.4
The Local Situation
Deaths due to CVD contributed towards 40% of all deaths in 2013 and represent the most common cause of death locally. This does not include deaths where the underlying cause of death is diabetes (usually represents between 3-5% of all deaths) where frequently, cardiovascular conditions also contribute to death.
In 2013, deaths due to circulatory diseases represented 42% of deaths in females and 39% of deaths in males, showing a similar, however smaller gender disparity as found in Europe. This gender disparity is mainly due to cerebrovascular diseases and other heart diseases (mainly heart failure), while in deaths due to ischaemic heart disease there was a male predominance.
While CVDs are still the commonest cause of death in Malta, they represented a much higher percentage of deaths in the past, where 60% of deaths in females and 55% of deaths in males were caused by CVD 30 years ago.
Over the past 30 years (figure 1), following an initial decline in the number of deaths due to CVD in both gender, the total number of deaths has remained stable over the past 25 years. The total number of deaths in 2013 was 1298 while the number of deaths in 1989 was 1316. As described previously when considering mortality from any cause one has to take into account the effect of population growth as well as the aging of the population, apart from other epidemiological changes in CVD.
The crude mortality rate which represents the total number of deaths from CVD divided by the total deaths and therefore is taking into consideration the increasing population size is showing a downward trend. However the greatest downward trend in cardiovascular mortality is being seen in the age standardised death rate in females despite the relative stable crude mortality rates from the early 1990s, indicating that people are dying at an older age.

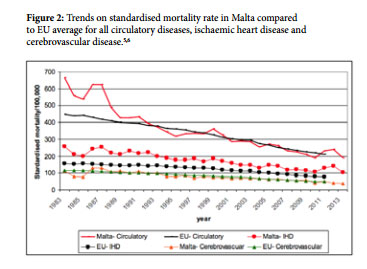
Rates for CVD mortality for Malta compare well with the EU average for all CVDs as seen in figure 2. Rates for cerebrovascular diseases are also similar to the EU average and have been so for the past 30 years. However rates for ischaemic heart disease are higher in Malta than the EU average, though the gap seems to be decreasing. In those countries where cancer supersedes cardiovascular mortality in males, all have lower mortality rates than Malta for circulatory disease.
Discussion
The natural history of cardiovascular epidemics, including coronary heart disease, varies markedly among countries. Different coronary heart disease patterns are distinguishable including ‘rise and fall’ (classic epidemic pattern), ‘rising’ (first part of epidemic) and ‘flat’ (no epidemic yet).7 Malta followed the ‘rise and fall’ epidemic with increasing cardiovascular mortality rates till the late 1970s-early 1980s followed by a fall from the 1980s onwards.
Mortality rates continue to fall in most but not all European countries. Geographic inequalities in cardiovascular mortality continue to exist in Europe with countries like Norway, Denmark, France, Portugal, Spain and the Netherlands having the lowest rates of cardiovascular mortality.3 Mortality rates generally appear to be most closely linked to a country’s stage of epidemiological transition. This refers to the changes in the predominant forms of disease and mortality burdening a population that occur as its economy and health system develops. Underdeveloped countries are still in the early stages of epidemiological transition where infectious disease predominates,8 whereas at the other end, in countries with late stages of epidemiological transition, cancer mortality is superseding cardiovascular mortality.
Studies examining the causes of the decline in CVD incidence and mortality in developed countries since the mid-1960s suggest that risk-factor reductions and treatment each account for between 40% and 60% of the reduction in CVD mortality, with undetermined causes accounting for an additional reduction of up to 10%.9,10
From a policy and intervention perspective, a decreasing mortality trend does not necessarily mean we are seeing less deaths due to circulatory conditions. Locally, due to demographic trends, though mortality rates from CVDs continue to decline, the actual number of deaths has remained stable for a number of years. It is also interesting to note that hospital discharges due to CVDs have increased locally from 665 per 100,000 in 2001 to 1341 per 100,000 in 2010,5 similar to the majority of European countries. This has obvious policy implications and emphasizes the continued high burden of CVD in European populations despite decreases in age-adjusted mortality rates.4