
Current weaning practices in a group of Maltese parents
Joseph Mizzi, Valerie Zammit
Abstract
Background
Certain weaning practices are known to increase the risk of problems such as allergies, fussy eaters and childhood obesity.
Aim To assess the variations in weaning practices, including the time of introduction of food and of lumpy/finger foods in a group of Maltese parents.
Methods Email questionnaire-based survey of the weaning practices of 300 parents.
Results There were 130 respondents. One-third of infants were exclusively breast fed. Two-thirds of parents started weaning between 4 and 6 months. Lumpy foods were introduced after eight months in 74% of cases. Conclusions Significant deviations from the recommended weaning advice were identified which potentially increases the risk of problems in these children.
Conclusions Significant deviations from the recommended weaning advice were identified which potentially increases the risk of problems in these children.
MESH terms: weaning, questionnaire, obesity
Introduction
Correct weaning practices are important to reduce the risk of allergies, the development of fussy eaters later on in life, and childhood obesity. Weaning practices in different countries vary greatly, but some principles are well established, namely, (a) exclusive breastfeeding till around 6 months of age, (b) the introduction of simple foods such as rice cereal, fruit and vegetables, followed later on by meat, eggs and dairy products, and (c) the introduction of lumpy foods and finger foods at around 8 months of age.
Objectives
The aim of this study is to assess the variations in weaning practices, including the time of introduction of food, and lumpy or finger foods, and thus to compare the results to the official recommendations by the Maltese Department of Health and other health authorities.
Methods
A deliberately simple and short questionnaire (Appendix 1) was sent by email to a cohort of 300 parents in March 2010, who were asked to return the completed questionnaire by email. It included questions on the timing of weaning, the types of food used, the introduction of solid and finger foods, and feeding habits. The email addresses were obtained over the previous two years from the parents of young infants in the private practice of one of the authors (JM), and they were all included in the study. Of the 340 parents asked to give their email address, forty did not have an email account.
Results
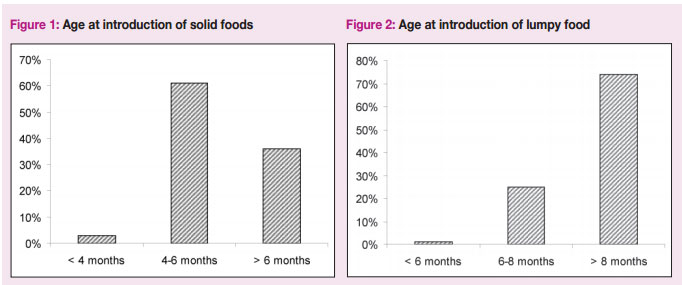
Of the three hundred questionnaires sent out, 130 (43%) were returned, most of the respondents were mothers (79%), aged between 31 and 40 (63%). The results are summarized in Table 1. Thirty-four percent of infants were exclusively breast fed. Most parents (61%) started weaning between 4 and 6 months; a few started before four months (Figure 1). Baby rice cereal was the first weaning food in the majority of babies (81%). Lumpy foods were introduced after eight months in 74% (Figure 2). Meat, chicken or fish were introduced at six to eight months in 59%, with 30% starting after 8 months. A number of parents (16 out of 130) sometimes added a biscuit to the bottle feed. Forty-three percent of babies were never or rarely fed during family meals. Parents obtained information about weaning from various sources, including their doctor, printed literature, internet, the midwife and the grandparents. Slightly more than half of the parents found weaning a pleasant experience, with the other half saying it was a challenging one. All the respondents were aware of the importance of appropriate hygiene practices when preparing feeds.
Discussion
This study has shown that there are clinical significant variations in the timing and other important aspects of weaning in a limited number of Maltese families. The number of exclusively breastfed babies was low (34%, compared to about 70.3% in Sweden in 2003)1 in spite of a national policy promoting breast feeding and the establishment of a Breast Feeding Clinic, which to date is still hospital-based and is limited by the number of personnel. The health benefits of breastfeeding include reduced risk of infectious diarrhoea and acute otitis media.2 Population-based studies have confirmed an association between breastfeeding and lower risk of obesity of the baby in later life; this association is stronger if the infant was exclusively breast-fed.3,4
Overall weaning was started according to current recommendations, which is around six months of age, with a tendency of many mothers to start as early as four months. This is acceptable. The WHO guidelines recommend ‘exclusive breastfeeding from birth to 6 months of age, and [to] introduce complementary foods at 6 months of age while continuing to breastfeed.’5 However, according to a recent re-evaluation of the current evidence by the European Society of Paediatric Gastroenterology, Hepatology and Nutrition (ESPGHAN), exclusive or full breast-feeding for about 6 months remains a desirable goal, but they clarify that complementary feeding should not be introduced before 17 weeks and not later than 26 weeks.6 The American Academy of Pediatrics also advices starting weaning between 4 and 6 months.7
The most common introductory food was rice cereal. Animal protein was introduced appropriately at around 6 months of age. There is no convincing scientific evidence that avoidance or delayed introduction of potentially allergenic foods, such as fish and eggs, reduces allergies, either in infants considered at increased risk for the development of allergy or in those not considered to be at increased risk.5 There is also no scientific basis for preferring one type of food to another as the initial weaning food – one may start a plain rice cereal, vegetable puree or fruit. Well-cooked eggs,8 fish9 and orange juice10 may be safely included in the infant’s diet from six months of age. Breast milk or formula milk should be the main milk source until 12 months of age, however small amounts of pasteurized cow’s milk may be added to the complementary food. Moreover, dairy products such as cheese and yogurt should be included in the infant’s diet.5
It is interesting to note that a number of parents added biscuits or cereals to milk in bottles despite the recommendation to use biscuits only as finger foods at an older age. A third of babies were not fed with the family, thus depriving the baby and other family members of the beneficial social interactions associated with sitting together at table.
Only 25% introduced lumpy food and finger food between 6 and 8 months of age. The late introduction of lumpy food or finger foods may result in feeding problems later on. Reduced consumption of important food groups such as fruits and vegetables, as well as feeding difficulties are more likely to occur when lumpy foods are introduced at or after 10 months of age.11,12
Parents obtain information from a variety of sources which are not always consistent and correct. The Department of Health has published a guide on weaning in English. To our knowledge there is no information on weaning available in Maltese, or any information about the subject on the Health Promotion website.
Weaning proved to be a challenging experience to a relatively high proportion of parents, perhaps reflecting on parental expectations and inexperience of those participants who were first-time parents. This observation would merit further evaluation in order to identify the greatest source of difficulty in handling this phase of parenthood.
The main limitations of the study are the small size and bias of the study population. The participants came mainly from the South Harbour and East regions of Malta. No attempt was made to classify them according to social class. Moreover their feeding and weaning practices were influenced by a single paediatrician. Therefore the results cannot be extrapolated to the entire Maltese population. This study has demonstrated a great variability of the weaning practices which differ from established recommendations and which are know to influence children’s health. This suggests a need for improving parental education which can be achieved by using a variety of media. Further research on a more representative sample of the Maltese population is suggested.
Table 1: Summary of participants’ data
• Parent’s sex: Mother 103 (79%); Father 27 (21%).
• Parent’s age: 20-30 42 (32%); 31-40 81 (63%); 41-50 7 (5%).
• Milk before weaning: Breast milk 44 (34%); Formula milk 33 (25%); Both 53 (41%).
• Biscuit added to milk in bottle: Yes 0 (0%); No 114 (88%); Sometimes 16 (12%).
• Information on weaning: Midwife 42 (32%); Doctor 80 (62%); Grandparents 20 (15%); Books/Magazines/Internet 68 (52%).*
• Age at first solid food: Less than 4 months 4 (3%); 4-6 months 79 (61%); More than 6 months 47 (36%).
• First weaning food: Baby rice cereal 105 (81%); Pureed vegetables 17 (13%); Pureed fruit 8 (6%); Other (0%).
• Introduction of meat/chicken/fish: Less than 6 months 14 (11%); 6-8 months 77 (59%); More than 8 months 39 (30%).
• Introduction of finger foods or lumpy foods: Less than 6 months 1 (1%); 6-8 months 32 (25%); More than 8 months 97 (74%).
• Baby fed during family meal times: Yes 74 (57%); No 25 (19%); Rarely 31 (24%).
• Weaning experience: Enjoyable 73 (56%); Challenging 57 (44%).
• Hygiene awareness: Yes 130 (100%); No 0 (0%). * adds to 210 since information could have been obtained from multiple sources
References 1 EUPHIX [Internet]. Breastfeeding; c2008 [updated 2009 Dec 17; cited 2010 Jun 19] Available from: http://www.euphix.org/ object_document/o4710n27421.html 2 Agostoni C, Braegger C, Decsi T, Kolacek S, Koletzko B, Michaelsen KF et al. Breast-feeding: A Commentary by the ESPGHAN Committee on Nutrition. J Pediatr Gastroenterol Nutr. 2009 Jul;49(1):112-25. 3 Singhal A, Lanigan J. Breastfeeding, early growth and later obesity. Obes Rev. 2007 Mar;8 Suppl 1:51-4. 4 Li R, Fein SB, Grummer-Strawn LM. Association of Breastfeeding Intensity and Bottle-Emptying Behaviors at Early Infancy With Infants’ Risk for Excess Weight at Late Infancy. Pediatrics. 2008 Oct;122 Suppl 2:S77-84. 5 Pan American Health Organization [Internet]. Guiding principles for complementary feeding of the breastfed child; c2003. [cited 2010 May 15]. Available from: http://www. who.int/child_adolescent_health/documents/ a85622/en/index.html 6 Agostoni C, Decsi T, Fewtrell M, Goulet O, Kolacek S, Koletzko B et al. Complementary Feeding: A Commentary by the ESPGHAN Committee on Nutrition. J Pediatr Gastroenterol Nutr. 2008 Jan;46(1):99-110. 7 American Academy of Pediatrics [Internet]. Switching To Solid Foods; c2010. [updated 2011, Jul 1; cited 2011, Jul 6]. Available from: http://www.healthychildren.org/English/ ages-stages/baby/feeding-nutrition/Pages/ Switching-To-Solid-Foods.aspx 8 NHS Choices [Internet]. Foods to avoid; c 2010 [updated 2009, Jul; cited 2010, Jun 12]. Available from: http://www.nhs.uk/Planners/ birthtofive/Pages/Foodstoavoid.aspx 9 NHS Choices [Internet]. Solids: the next steps; c2010 [updated 2009, Jul; cited 2010, Jun 12]. Available from: http:// www.nhs.uk/Planners/birthtofive/Pages/ Solidsthenextsteps.aspx 10 NHS Choices [Internet]. Drinks and cups; c2010 [update 2009, Jul; cited 2010, Jun 12]. Available from: http://www.nhs.uk/Planners/ birthtofive/Pages/Drinksandcups.aspx 11 Coulthard H, Harris G, Emmett P. Delayed introduction of lumpy foods to children during the complementary feeding period affects child’s food acceptance and feeding at 7 years of age. Matern Child Nutr. 2009 Jan;5(1):75-85. 12 Northstone K, Emmett P, Nethersole F. The effect of age of introduction to lumpy solids on foods eaten and reported feeding difficulties at 6 and 15 months. J Hum Nutr Diet. 2001 Feb;14(1):43-54.