
Colonoscopy Screening in Moderate
Clayton John Fsadni, Sarah Caruana Galizia & Morolayo Owolabi
Abstract
Colorectal cancer is one of the commonest forms of cancer in the Maltese population. It can be treated successfully if detected early. Education and screening are the major components of early detection. The aim of this study was to determine the pattern of colonoscopy screening in patients at moderate risk of developing colorectal cancer in a surgical firm at Mater Dei Hospital. 90 patients that fit into the moderate risk category were identified from the firm’s endoscopy database. The pattern of screening was then compared to the NICE guidelines. It was found that colonoscopy screening was more aggressive than recommended by the NICE guidelines.
Introduction
Colorectal cancer (CRC) is one of the commonest cancers in the Maltese population but can be treated successfully if detected early. The major components of early detection are education and screening.1
People with a family history of CRC but with no genetic disorder putting them at high risk of CRC are considered to be at moderate risk of developing CRC. These are further divided into high-moderate and low-moderate risk subcategories. The preferred surveillance mode for patients with a moderate risk of developing CRC is total colonoscopy.2
The aims of this audit are to:
- Evaluate the colonoscopy screening pattern for individuals with a family history indicating moderate risk for CRC in a surgical firm at Mater Dei Hospital.
- Compare this pattern with that recommended by the NICE guidelines.
Methodology
Setting and Data Collection
This retrospective study was conducted at Mater Dei Hospital between April – June 2015 within a surgical firm that records its endoscopic services on iSOFT, which is a secure database utilised at Mater Dei Hospital.
A total of 90 patients having one or more first degree relatives (FDRs) affected by colorectal cancer who had undergone at least one colonoscopy between November 2007 – January 2015 were identified. Their respective age, indication for colonoscopy, date of procedure and findings were retrieved from the database.
These patients were then phoned and asked about:
- The number of relatives and degree of relation of relatives affected by CRC;
- Age of relative/s at time of diagnosis with CRC;
- Presence of gastrointestinal – related symptoms prior to colonoscopy;
- Number of colonoscopies and the respective dates at which they were performed;
- Any other investigative procedures done for the same condition.
Compliance for each parameter was awarded a 25% score. Compliance to all categories was given a 100% compliance. The average percentage compliance was then calculated for all patients within each risk category. Any discordance between the guidelines and actual practice was recorded.
Standard Used
The guidelines used were the NICE Guidelines for colorectal cancer screening and surveillance in moderate risk family groups.2 These were updated by The British Society of Gastroenterology (BSG) and the Association of Coloproctology for Great Britain and Ireland (ACPGBI) in 2002.
Data Analysis
All data were processed using Microsoft Excel 2013 and analysed by comparing the number of colonoscopies performed between November 2007 – January 2015 for every patient, with the screening procedure and respective interval recommended by the NICE Guidelines.2 The parameters required to assess compliance with guidelines included:
- The number of first degree relatives affected;
- Age of diagnosis of such relative/s;
- Age of patient at which colonoscopy was first undergone;
- Number of colonoscopies within a 5 year interval.
Any discordance between the guidelines and actual practice was recorded.
Ethical approval and consent
The study was approved by the Audit and Data Protection Act Committee and the Mater Dei Hospital data protection Unit. Consent was obtained from the Consultant Surgeon of the Firm.
Results
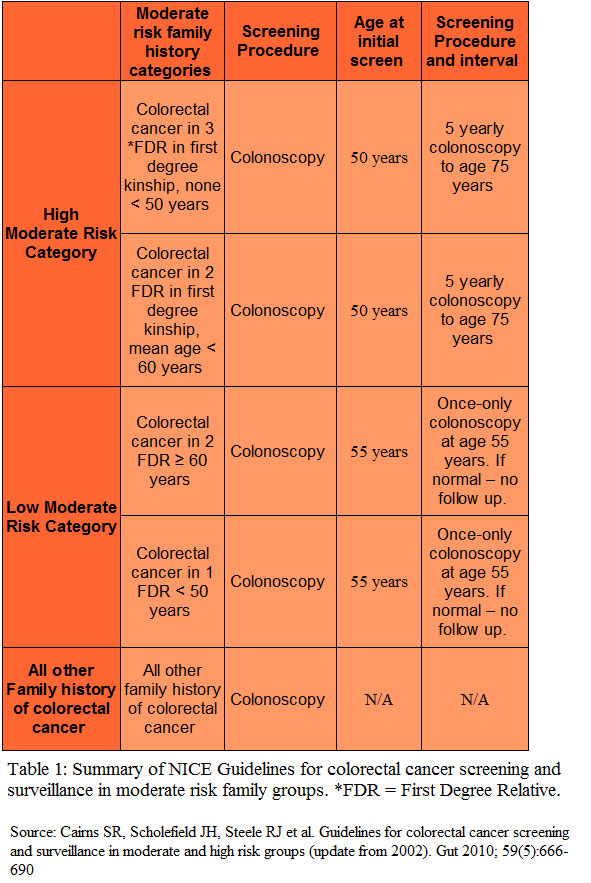
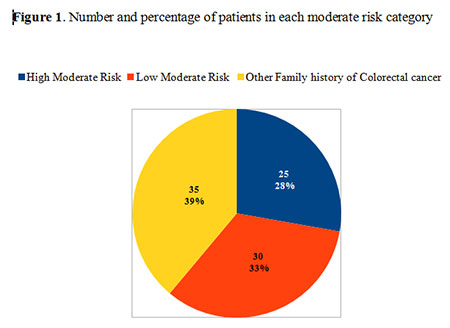
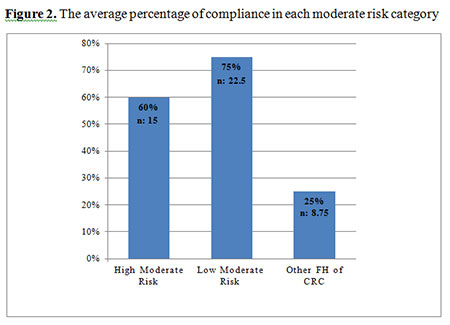
A summary of the NICE guidelines for colorectal cancer screening and surveillance is shown in Table 1. As shown in Figure 1 the greatest number of patients fell in the ‘other Family history of CRC category’, (35 from 90 patients; 39%). Average compliance to the NICE guidelines was greatest in the low moderate risk category (75%) while the lowest compliance was observed in the other family history of CRC category (25%), as shown in Figure 2.
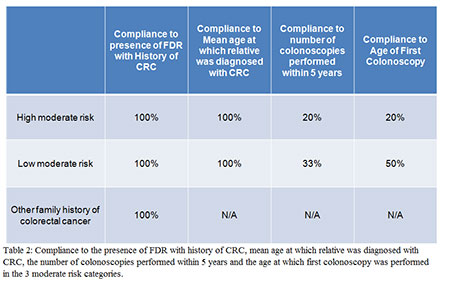
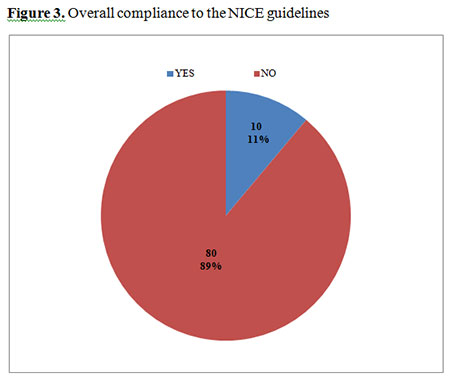
There was 100% compliance in all categories to the NICE recommendations pertaining to the screening process of patients with FDR having a history of CRC (Table 2). Compliance to mean age at which relatives were diagnosed with CRC was 100% in the high moderate risk and low moderate risk categories. All the patients screened had one or more first degree relatives with history of colorectal cancer, so compliance to this parameter was fulfilled in all categories. The mean age at which the affected relatives were diagnosed with colorectal cancer was also complied with in the low moderate risk category and high moderate risk category. However, compliance to the recommended frequency of screening and age at which to start screening was low in all categories. Overall percentage compliance to the NICE guidelines across all categories was 11% (Figure 3).
Discussion
Family history categories and recommendations
A positive family history of CRC confers an increased risk for the development of CRC.3
The study considered the moderate risk category which is further divided into high moderate risk and low moderate risk. The remaining patients fell into the ‘other family history of CRC’ category.
i. The high moderate risk category1 includes:
1. Patients with 3 or more affected relatives in a first degree kinship with each other (none <50 years old as otherwise they would fulfil high risk criteria).
2. Two affected relatives with a mean age < 60 in a first degree kinship.
Recommendation
In this category patients merit low intensity surveillance comprising 5 yearly colonoscopy commencing at age 50 and continuing till 75 years of age. Polyps must be snared and histologically characterised. If adenomas are present, surveillance should be instigated as per adenoma surveillance guidelines.2
ii. The low moderate risk category1 includes:
1. Patients with only one affected relative < 50 years old.
2. Patients with only two affected first degree relatives aged 60 years or older.
Recommendation
Once only colonoscopy at 55 years of age. Polyps must be snared and histologically characterised. If adenomas are present surveillance should be instigated as per adenoma surveillance guidelines.2
iii. All other family history of CRC1
Recommendation
No need for screening.
Compliance with screening recommendations
Most patients screened had a family history of CRC but did not fit the criteria for low or high moderate risk. The highest average percentage compliance (75%, n = 22.5) was found in the low moderate risk category (Figure 2).
a. Compliance in the High Moderate Risk Category
In the high moderate risk category, full compliance was observed with regards to the NICE criteria relating to the screening of patients that had first degree relatives with a history of CRC as well as the mean age at which the relatives were diagnosed. Compliance was not observed with regard to the number of recommended colonoscopies as there was a tendency to screen every 2 years rather than the recommended 5 year interval. When it came to the age of first colonoscopy, delayed and early screening initiation were equally observed. Unawareness of the guidelines, practice of defensive medicine and pressure from patients could all be reasons for non-compliance.
b. Compliance in the Low Moderate Risk Category
Most patients in this category had more colonoscopies than recommended by the guidelines. Reasons for this may be similar as for the high – moderate risk category, that is inadequate history taking leading to improper categorisation of patients, unawareness of the guidelines and the practice of defensive medicine by the clinician. Pressure from the patient and/or relatives, mainly due to anxiety and insecurity may also have contributed to this.
With regards to the age at which screening was initiated, non-compliance was due to delayed screening initiation rather than early screening initiation. Delayed screening initiation may occur if the patient is not under the care of a primary health care provider at the time at which screening is supposed to start. Primary health care providers have an important role to play in advising patients when they should have their first screening colonoscopy as advised by guidelines and according to which risk category they are in. Another reason for delayed screening initiation is that the patient may be older than the recommended age for screening initiation by the time CRC is discovered in his / her relatives. Health care providers’ lack of knowledge of the screening guidelines may also contribute to delayed screening initiation.
c. Compliance in Patients with ‘Other Family History of CRC’
According to the NICE guidelines, screening is not recommended for those patients with a family history of CRC that did not fall into either of the above categories. Hence, these patients should not have had a colonoscopy. The study showed that screening was mainly conducted on the basis of whether the patient had a first degree relative with a history of CRC or not. The main reasons for non-compliance in this category are the same as the ones mentioned for the previous categories, that is, limited sampling units, pressure to perform screening by the patient or relatives, the practice of defensive medicine and the possible belief of some clinicians that the guidelines for screening are not stringent enough and that following them may lead to missed cases of CRC.
As for any other guidelines, dissemination, accessibility, clarity and regular updating of guidelines is essential to ensure clinician awareness and to improve compliance.
Outcomes of the Screening Colonoscopies Performed
Across all categories, in 50% (n = 45) of the colonoscopies carried out, no abnormality was detected (Figure 4).
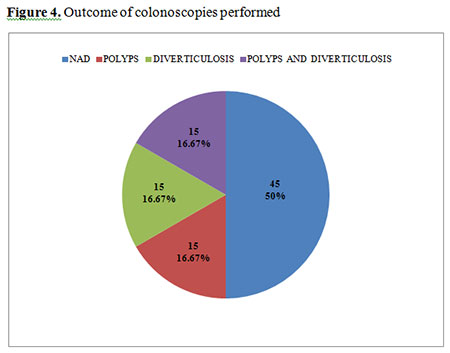
Of the patients that did not fall into low or high moderate risk categories, only 14% had polyps on colonoscopy. This supports the recommendation of the guidelines that screening is not to be performed in this category of patients.
It is suggested that left-sided hyperplastic colonic polyps (generally within the reach of a screening sigmoidoscopy) serve as a marker for neoplastic polyps.4
Limitations
The main limitations were:
a. The cohort of patients all belonged to the same surgical firm;
b. The small sample size;
c. The patients may have forgotten certain details by the time of interview;
d. Time constraints limited the assessment of the overall survival in all referrals according to their risk category.
Conclusion and recommendations
The tendency is to screen more aggressively than recommended by the NICE guidelines, possibly due to inaccurate history taking and improper patient categorization, unawareness of the guidelines, the practice of defensive medicine and pressure from anxious patients and relatives. To improve compliance, it is recommended that the NICE guidelines should be easily accessible, clear, well-disseminated and regularly updated. There should be more clinician awareness of the unnecessary stress, inconvenience and discomfort that excessively aggressive screening can cause to patients. In patients that fell into the ‘other family history of CRC’ category, polyps were only found in 14%, supporting the guidelines’ recommendation that screening is not necessary in these patients.
References
- National Colorectal Cancer Screening Programme. Ministry of Health, Elderly and Community Care. Available from: https://healthcms.gov.mt/en/phc/nbs/Pages/Colorectal-Screening-Programme.aspx
- Cairns SR, Scholefield JH, Steele RJ et al. Guidelines for colorectal cancer screening and surveillance in moderate and high risk groups (update from 2002). Gut 2010; 59(5):666-89. Available from: http://www.nhslothian.scot.nhs.uk/Services/A-Z/EndoscopyUnit/InformationForClinicalStaff/Documents/BSGCRCancerSurv2010.pdf
- Otto L. Colorectal cancer screening in patients at moderately increased risk due to family history. World J Gastrointest Oncol 2012; 4(6):125-30.
- Ansher AF, Lewis JH, Fleischer JE et al. Hyperplastic colonic polyps as a marker for adenomatous colonic polyps. Am J Gastroenterol 1989; 84(2):113-7.