
Cardiac surgery in Malta: past, present and future
Alexander Manché
Abstract
In 1918 neurosurgeon Sir Charles Ballance removed a bullet from the heart of a soldier based in Malta. After WWII cardiac surgeon Mr Lance Bromley and cardiologist Dr Edwin Besterman treated Maltese patients in St Mary’s Hospital, London. A visiting consultant service in 1983 was followed by a permanent resident program in 1995, providing a comprehensive adult cardiothoracic service. The future of cardiac surgery depends on evolving technologies and surgeons who are innovators.
Cardiac surgery was inaugurated in Malta on the 16th February 1918 when Sir Charles Ballance, a renowned neurosurgeon and a colonel in the British Expeditionary Forces in Malta, removed a bullet from the heart of 21-year old trooper Robert Hugh Martin.1 Dr Sarah Marguerite White assisted Ballance and Lt Colonel Shirley administered the anaesthetic. The heart was exposed via a Kochers incision with removal of the left 4th to 6th costal cartilages. Charles Ballance cut into the right ventricle and retrieved the bullet with an artery forceps from the inferior interventricular septum adjacent to the apex of the heart. Significant haemorrhage was stemmed with internal Lembert sutures and a blood transfusion was also administered.2 This was the third such attempt worldwide but the patient died of sepsis one month post-operatively and the operation never achieved its due recognition. Ballance observed “it is a common experience that bullets frequently lodge in the tissue and induce neither local nor general infection until attempts at removal are made”. Ballance recorded his experience in the prestigious Bradshaw lecture, entitled The Surgery of the Heart, which he delivered the following year.3
The next milestone came in 1947 when Professor Peter Paul Debono operated on 8-year old Iris Magro of Naxxar and successfully ligated her patent ductus arteriosus. The operation was performed on the 27th September at the Bugeja Hospital, Hamrun; the first assistant was Dr Victor Griffiths and the anaesthetist Dr Joseph Darmanin Demajo. The patient was referred by Peter Paul’s brother, Professor Josie Debono and by Dr Victor Captur. She complained of weakness and lethargy and had a fever of up to 102°F. Examination revealed a machinery murmur in the pulmonary area and blood cultures were repeatedly positive for Streptococcus viridans. A presumptive diagnosis of infective endarteritis of the patent ductus warranted urgent surgery. At operation the left chest was entered via the second interspace, with division of two adjacent ribs. The ¾ inch ductus was identified and a silk ligature was passed over an aneurysm needle. The ductus was tied on its aortic side using a Ballance knot.4
The post-war years saw a consolidation of the links with the United Kingdom in the field of cardiology and cardiac surgery. Visiting consultants from London came to Malta on a regular basis to see patients and advise on treatment. Some of these patients would then be sent to St Mary’s Hospital London for further investigation and, in some cases, surgical treatment. Foremost amongst these visitors were cardiac surgeon Mr Lance Bromley and cardiologist Dr Edwin Besterman. Bromley and Besterman reported on their 14-year experience in Malta, performing closed mitral valvotomy at a mean annual rate of 4/100,000 population.5 Their standard technique, developed at St Mary’s Hospital London, involved commissurotomy using a Tubbs dilator. This London series, comprising over 500 patients over a 24-year period yielded excellent clinical results with 94% of patients enjoying full functional capacity, and less than 4% requiring reoperation at 10-year follow-up.6
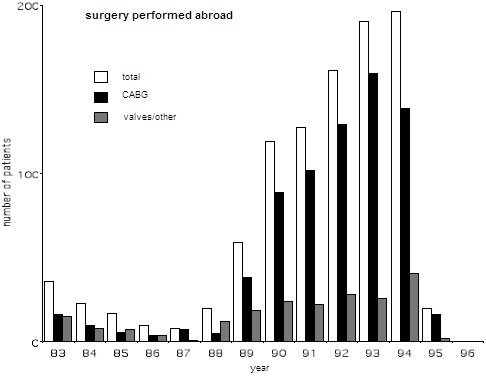
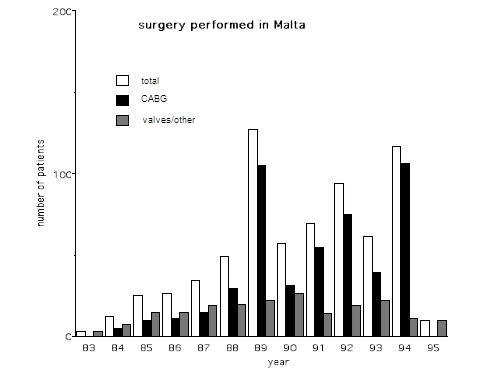
In 1983 Mr Alan Yates performed the first heart operation in Malta and inaugurated a visiting service here. Over the years Maltese patients benefited from the services of UK teams who performed surgery both in the UK (figure 1) and in Malta (figure 2). Yates was joined by Mr David Anderson, also from Guy’s Hospital. Other teams participating in this program were headed by Mr Rex Stanbridge from St Mary’s Hospital, Mr Fik Shabbo and Mr John O’Riordan from the Brook Hospital, Mr Alan Wood from the Royal London Hospital, as well as Mr Brian Fabri from Liverpool. The early 1990’s ushered in an expansion in terms of numbers and this provided a catalyst for setting up a permanent local cardiothoracic unit.
The author visited Malta in January 1995 and performed a trial series of 10 patients. Following his appointment as consultant cardiothoracic surgeon, and anticipating the arrival of cardiologist Professor Albert Fenech from the UK, the permanent local program was planned to commence in April 1995. In preparation for a smooth start in Malta, local theatre, intensive care and ward nurses were flown to the Northern General Hospital, Sheffield for clinical training. Major equipment that was purchased around this time included a heart-lung machine with heater/cooler unit, a blood gas analyser, theatre and transfer monitors, a servo ventilator, an intra-aortic balloon pump, syringe drivers, surgical instruments, as well as pump sets, oxygenators and heart valves. Based on the intervention rates in 1993 and 1994, both with regard to angioplasty and surgical operations, and taking into account the size of the Maltese population and the waiting list as it stood in January 1995, it was projected that approximately 350 operations would have to be performed annually in order to provide an effective service.
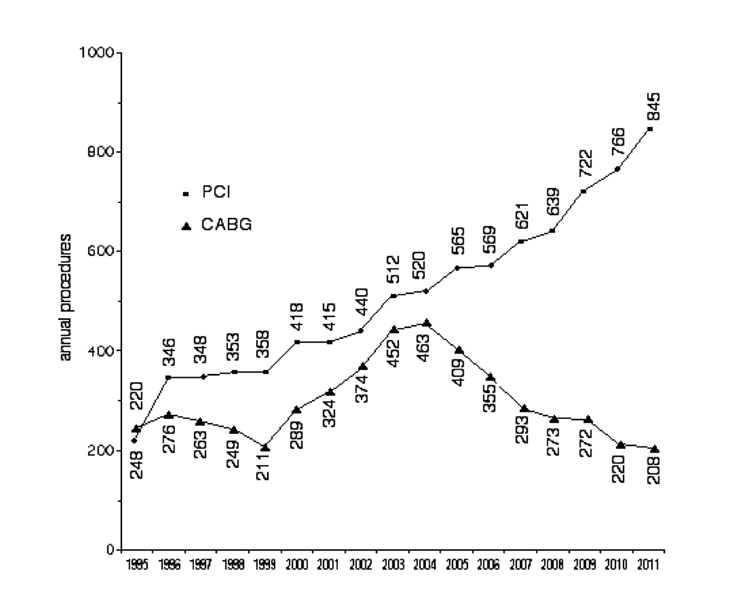
With the steady encroachment of interventional cardiology into the traditional cardiac surgical domain, the size and nature of our practice has evolved, and our current practice bears little resemblance to that of twenty years ago. A number of comparisons are highlighted in table 1 .
| 1995 | 2000 | 2015 | |
| Mean age | 60.7 | 64.9 | |
| Mean waiting time (weeks) | 38 | 2 | |
| Parsonnet risk | 7.6 | 11.6 | |
| EuroSCORE risk+ | 2.7 | 4.3 | |
| Coronary Artery Bypass Grafting | 82.7% | 44.2% | |
| Aortic Valve Replacement | 10.0% | 37.2% | |
| Mitral repair | 0* | 63.2%* | |
| Miscellaneous procedures | 1.3% | 7.0% | |
| Mean post-op length of stay (days) | 6.46 | 7.51 | |
| Post-op Atrial Fribrillation | 7.0% | 36.4% |
+ EuroSCORE was calculated from 2000 onwards; *denotes % of mitral procedures
Table 1. Comparison of evolving nature of cardiology services in Malta
The future of cardiac surgery in Malta is largely influenced but international trends. Continuing professional development, including conferences, seminars, hands-on hospital visits, proctoring, and most importantly, the training of our future surgeons in large units abroad, will assure the maintenance of a high quality service. Our relatively small unit provides a diverse and comprehensive cardiothoracic service comparable with that in larger countries. The immediate challenges facing our surgeons involve advances in the fields of surgery for atrial fibrillation,9 more complex mitral valve repair,10 corrective surgery for annulo-aortic ectasia,11 and minimally invasive cardiac and thoracic procedures. To guess the evolution of cardiac surgery in the distant future is to venture into the unknown. What is sure is that more collaboration with interventionists is essential, and the future cardiac surgeon must be trained in open as well as percutaneous skills.12,13
References
1. Stone JL. Sir Charles Ballance: pioneer British neurological surgeon. Neurosurgery 1999;44:610-631.
2. White M, Ballance C. A case of removal of a rifle bullet from the right ventricle of the heart. J Roy Army Med Corps 1918; 31(4):484-496.
3. Ballance CA. (1920) The Bradshaw Lecture on the surgery of the heart. London. Lancet 1924;1:134.
4. Manché A, Grech V. Early cardiac surgery in Malta. Malta Med J 2012;24:42-44.
5. Besterman E, Bromley LL. Mitral valvotomy – value of the closed technique. BMJ 1980;280:563.
6. Besterman E. Mitral valve commissurotomy. Am J Cardiol 1984;53:1488.
7. Manché A. Early and late outcomes after heart transplantation in a low-volume transplant centre. Malta Med J 2012;24:30-34.
8. Manché A, Casha A. Are percutaneous coronary interventions changing our coronary surgery practice? Malta Med J 2011;22:19-23.
9. La Meir M. Surgical options for treatment of atrial fibrillation. Ann Cardiothorac Surg 2014;3:30-37.
10. Fedak PWM, McCarthy PM, Bonow RO. Evolving concepts and technologies in mitral valve repair. Circulation 2008;117:963-974.
11. Cozijnsen L, Braam RL, Waalewijn RA, Schepens MA, Loeys BL, van Oosterhout FM, et al. What is new in dilatation of the asceding aorta? Circulation 2011;123:924-928.
12. The Advisory Board Company. What’s the future of cardiac surgery? How it will affect your CV program. February 11, 2014. Available from: www.advisory.com/research/service-line-strategy-advisor/expert-insights/2014/whats-the-future-of-cardiac-surgery
13. Verrier ED. The future of cardiothoracic surgery …dying star or supernova? American Association for Thoracic Surgery. 2013. Available from: http://aats.org/TSR/Cardiothoracic-Surgeon/The-Future-of-Cardiothoracic-Surgery.cgi