
Blepharitis
James Vassallo & Suzanne Pirotta
Blepharitis is a very common and under-appreciated eyelid margin condition which causes non-specific ocular irritation, significant patient distress. Chronic blepharitis is often difficult to manage. The true prevalence of blepharitis is difficult to estimate; figures cited in the literature range from 12%-79% due to the different ways how blepharitis may manifest itself and ill-defined diagnostic criteria.1
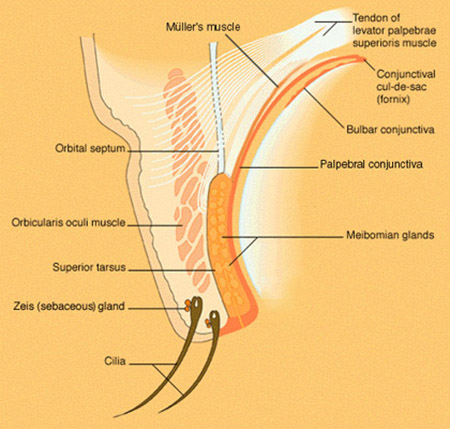
Blepharitis can be classified in several ways – the anatomical classification is probably more useful clinically (Figure 1). The disease is usually bilateral and can be divided into anterior and posterior blepharitis.2
The pathophysiology of blepharitis is multifactorial and bacteria play a central role.3 The most common organisms cultured from blepharitic lids are Streptococcus epidermidis (96%), Proprionibacterium acnes (93%), Corynebacterium sp. (77%) and, Staphylococcus aureus (49%). Anterior blepharitis is mostly bacterial, either due to direct infection, toxin-mediated reactions, or due to a hypersensitivity reaction to bacterial antigens. Posterior blepharitis is associated with underlying structural and functional changes of the meibomian glands, hence the term meibomian gland dysfunction (MGD). The mechanism of posterior blepharitis may also be due to the presence of bacteria, specifically via the production of lipases which alter the components of the meibum. This process may ultimately lead to glandular obstruction and formation of internal hordeola and chalazia. Lack of normal lipid secretion from the meibomian glands leads to many of the symptoms reported by patients. Demodex mites are an overlooked cause of anterior and posterior blepharitis and should always be considered in recalcitrant cases, lash abnormalities and cylindrical dandruff, and recurrent chalazia.4 Other aetiological factors include seborrhoeic dermatitis (associated with Demodex folliculorum infestation), ocular acne rosacea, and isotretinoin.2,5
Patients often complain of non-specific irritation, burning or foreign body sensation, itching, watery and red eyes, crusting, mild discharge and a fluctuating blurring of vision. Symptoms tend to be worse in the morning and their severity does not always correlate with the severity of the underlying blepharitis.4 The manifestations of the disease may be asymmetrical but features of a unilateral blepharitis should always prompt the examining doctor to consider other pathologies which may mimic this condition, primarily, sebaceous gland carcinoma.5 Other differential diagnoses include lid infections, hypersensitivity reactions, and discoid lupus. Some normal age-related changes, such as mild telangiectasia, may be erroneously attributed to blepharitis.2
External examination of the lid in blepharitis shows thickening, scaling, swelling, redness and eyelash abnormalities.5 Under the higher magnification of the slit lamp other features of anterior blepharitis include lid telangiectasia, greasy matted lashes, collarettes around the bases and sleeves along the shafts of the lashes (Figure 2). In posterior blepharitis, there is pouting of meibomian gland orifices from which thickened lipid secretions may be expressed together with a frothy tear film (Figure 3).4
Severe chronic blepharitis may lead to several lid and corneal complications (Table 1). Intraocular procedures such as cataract surgery in a patient with blepharitis are associated with a higher risk of infectious endophthalmitis.6
| Lid
|
Cornea |
| Recurrent chalazia | Dry eyes |
| Scarring | Recurrent erosions |
| Punctal misdirection | Bacterial keratitis |
| Trichiasis (inward misdirected lashes) | Marginal keratitis |
| Madarosis (lash loss) | Contact lens intolerance |
| Poliosis (whitening of lashes) | Scarring |
| Perforation (rare) |
Table 1. Lid and corneal complications associated with severe chronic blepharitis
This is a challenging condition to manage and one must start by educating the patient about the disease itself as the patient needs to have an active role in the treatment. Investing time in education early on will help improve compliance, achieve realistic expectations, and maximize outcomes. Combination treatment tailored for the individual patient with a trial and error approach is often needed.7
Management of this problem includes both non-pharmacological and pharmacological options. The former focuses on eyelid hygiene and mechanical methods to decrease bacterial load and improve meibomian gland function thus decreasing inflammation and restoring the natural tear film. Mechanical methods include lid scrubs, warm compresses and lid massage. There are commercially available products dedicated for this purpose, or else the patient may use simple items such as diluted baby shampoo, cotton wool, and warm face towels. Since most patients with blepharitis have dry eyes, lubricating drops should be prescribed and there are formulations specifically designed for MGD.
Topical antibiotic ointment, with or without a steroid, applied to the lid margin may be needed. The treatment regimen is individualised according to disease severity and patient response. Steroid use should be minimised and topical cyclosporine is an alternative (not available locally). Long- term antibiotic treatment may lead to antimicrobial resistance and therefore the antibiotics used should be changed regularly.
For patients not responding to treatment, especially those with MGD, oral tetracyclines or macrolides may help. The diagnosis of Demodex infestation should be considered in such cases and treatment of this includes metronidazole gel (locally available preparations are licensed for cutaneous use and contact with the eyes should be avoided), tea tree oil preparations, and oral ivermectin.
Significant symptomatic improvement generally takes several weeks unless it is due to acute infection, in which case it may resolve with appropriate antibiotic therapy.8 It is of utmost importance that the patient and caring doctor realize that blepharitis is generally a chronic condition which has to be controlled long-term and is not curable. This understanding can help minimize patient and doctor dissatisfaction that is often associated with the management of the condition.
It is important to keep blepharitis in mind when assessing children with chronic red eyes, irritation and recurrent chalazia in order to prevent corneal complications, which in children may be amblyogenic. Treatment is mostly the same as for adults, with erythromycin being used instead of tetracyclines when an oral antibiotic is needed.9
As with other chronic conditions, blepharitis is associated with anxiety and depression and so decreases the health-related quality of life. In patients who are failing to improve, presenting repeatedly, or not complying with treatment, an underlying psychological issue must be considered.10


References
1. Lindstrom RL, et al. Blepharitis – Update on research and management. The NewYork Eye and Ear Infirmary Institute for Continuing Medical Education. 2010.
2. Kanski JJ. Clinical Ophthalmology – A systematic approach. 6th edition. Philadelphia: Elsevier Butterworth Heinemann; 2007. Chapter 4, Eyelids; p.128-131.
3. BMJ best practice – Blepharitis [Internet] 2015 [updated 2015 Jan 5; cited 2015 Jan 7]. Available from: http://us.bestpractice.bmj.com/best-practice/monograph/574.html
4. Jingbo L, Hosam S, Scheffer CGT. Pathogenic role of Demodex mites in blepharitis. Curr Opin Allergy Clin Immunol. 2010 October; 10(5): 505–10.
5. Ganatra JB, Goldstein MH. Yanoff M & Duker JS Ophthalmology. 3rd ed. Mosby Elsevier; 2009. Chapter 4.4, Blepharitis; p.219-21.
6. Stead RE, Stuart A, Keller J, Subramaniam S. Reducing the rate of cataract surgery cancellation due to blepharitis. Eye. 2010; 24:742.
7. American Academy of Ophthalmology Cornea/External Disease Panel. Preferred Practice Pattern® Guidelines – Blepharitis. San Francisco, CA: American Academy of Ophthalmology; 2008. Available from: http://www.aao.org/ppp
8. Rapuano CJ. Color Atlas & Synopsis of Clinical Ophthalmology – Wills Eye Institute – Cornea.. 2nd ed. Lippincott Williams & Wilkins; 2012. Chapter 1, Conjunctival infections and inflammations; p.2-3.
9. Viswalingam M, Rauz S, Morlet N, Dart JKG. Blepharokeratoconjunctivitis in children: diagnosis and treatment. Br J Ophthalmol. 2005; 89:400–403
10. Chiang CC, Lin CL, Tsai YY, Peng CL, Liao YT, Sung FC. Patients with blepharitis are at elevated risk of anxiety and depression. PLoS ONE. 2013; 8(12):e83335.