
Audit on A-scan use prior to Cataract Surgery in Mater Dei Hospital
David Agius, Stefan Buttigieg, Obafemi Giwa Amu, Maria De Bono, Mario Vella
Background The A-scan is a method of measurement of the ocular axial length (L). It is coupled with corneal curvature keratometry (K) readings so that one can measure the required power (P) of an intraocular lens (IOL) used for cataract surgery. The Sanders, Retzlaff and Kraft (SRK) formula calculates the required P of the IOL as P = A − 2.5L − 0.9K where A is the specific IOL constant. The power of the lens determines the refraction of the image onto the retina and thus determines the visual acuity of the eye. The axial length of the eye is measured by the time a signal takes to be reflected back to the source, like ultrasound or light. Distance is calculated by the velocity formula, depending on the speed of the signal.1 In Mater Dei hospital, two methods are used to determine the axial length of the eye prior to cataract surgery, namely an ultrasound method and an optical method.
Aim To assess the proportion of use of each A-scan method, identify whether they are yielding different results and see whether one should be used over the other.
Method
This is a retrospective audit where notes from post-operative refraction visits were used in order to check the A-scan method, i.e. ultrasound method vs optical method, and the postoperative visual acuity and refraction. The notes of post-operative refractions done from November to December 2014 were taken into account.
Results
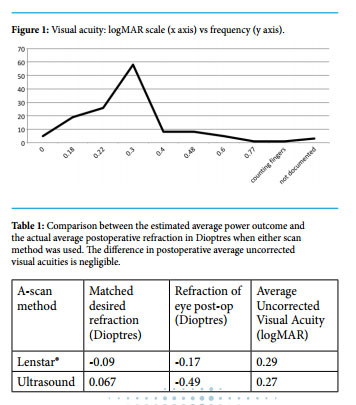
97% of the 135 patients that were operated under local anaesthesia and the majority of the patients undergoing cataract surgery were female (57%). 55% of the A-scans were performed using the Lenstar® optical technology while 38% were performed using the ultrasound method. The remaining 7% had both modalities used. No major difference was noted between the post-operative refraction and resulting visual acuity of these two types of scans. Figure 1 shows the wide range of visual acuities identified following the surgeries performed using both methods of A-scan. The logMAR scale was used. The mode for the Visual Acuity was 0.3 which is equivalent to 6/12 on the Snellen chart. The average visual acuity and refraction post-surgery for each patient was calculated and linked to the A-scan method which was previously used. Table 1 shows that there is no such difference in the post-operative visual acuity when either A-scan method is used.
Discussion
It is found out that both A-scan methods yield similar results in Mater Dei Hospital. Similar findings were also reported by Naicker et al.2 These two techniques are equally useful especially when considering the fact that they make up for each other’s disadvantages. The ultrasound method is invasive and can transmit infections because of direct eye contact but has the advantage that it works better than the Lenstar® with an uncooperative patient who cannot fixate his eyes on the machine. It is also better than the Lenstar® when it comes to dense subcapsular cataracts.3 The optical method is on the other hand preferable in shorter eyes.1 The use of ultrasound is also dependant on the user experience. However, Findl et al found no differences in outcomes between the ultrasound and the optical method as long as the user using the ultrasound method is experienced.4
Conclusion
Both A-scan techniques give similar post-operative visual acuities. They are equally useful since they accommodate different scenarios in view of their advantages and disadvantages.
{kind=link}