Audit of the aetiological factors of constipation leading to admission at Gozo General Hospital
Catriona Zammit, Christine Vella & Rachel Abela
Abstract
Constipation accounted for 2.31% of admissions at Gozo General Hospital in 2012. This audit was primarily designed to identify populations affected and causative aetiological factors. A secondary aim was to determine practices that required modification with a view to improve community management of the condition and thus possibly reduce unnecessary admissions.
Introduction
Constipation constituted 2.31% of admissions at Gozo General Hospital (GGH) in 2012 accounting for 148 days (0.65%) of total adult bed occupancy. This study looked at the causes of constipation in these patients and examined how these admissions could be minimized by being diagnosed and managed better in the community setting.
As described by Addison et. al,1 in a similar study carried out by a group at Harvard University, polypharmacy and inappropriate use of laxatives were a significant contributing factor predisposing to increasing constipation admissions. Another study by Hertzberg2 showed that many communitybased patients were poorly controlled even though they were receiving laxatives regularly. This was also shown to increase burden on NHS resources.
A better approach at handling constipation in the community setting will decrease the amount of hospital admissions which can be very distressing both to patients and their relatives and carers. Moreover, patients would benefit from not undergoing any inconvenient procedures such as enemas and not being exposed to the hospital environment which in itself predisposes the patient to a higher rate of infections.
Methodology
Patients admitted to GGH with constipation between 1st January 2012 and 31st December 2012 were identified from the GGH Hospital Activity Data. Patient files for the relevant admission were reviewed. Previous case notes were also reviewed for any relevant data. In total, 58 admissions for 57 patients were reviewed (one patient was admitted twice). Those deceased were excluded.
The following data were reviewed:
1. Age and sex of the patient
2. Structural and functional colonic and intestinal conditions possibly contributing to constipation including: • Past abdominal surgery • Irritable bowel syndrome • Anal fissures
3. Lifestyle factors: • Dietary habits – inadequate fibre intake, overuse of caffeine or alcohol, intake of large amounts of dairy products • Dehydration / Poor water intake • Immobility issues – being bed-bound, having arthritis, using wheelchairs • Stress
4. Medical Conditions: • Hypercalcaemia • Hyperparathyroidism • Hypokalaemia • Hypothyroidism • Diabetes mellitus • Neurologic Disorders – stroke, Hirschsprung disease, Parkinson’s disease, multiple sclerosis, spinal cord lesion, head injury, cerebrovascular accidents, Chagas disease, familial dysautonomia • Connective tissue disorders – scleroderma, amyloidosis, mixed connective-tissue disease • Psychological issues – depression, anxiety, somatisation and eating disorders 7
5. Medications • Antidepressants • Anticholinergics • Opioids • Calcium channel blockers • Diuretics • Psychotropic drugs (excluding antidepressants) • Cholestyramine and stimulant laxatives (long-term use) & stool softeners • Other medications including metals e.g. iron supplements, NSAIDs, sympathomimetics e.g. pseudoephedrine, antacids, oral contraceptives, thalidomide, calcium supplements.
In order to investigate any faecal loading, the patients’ electronic records were reviewed to analyse the investigations carried out on admission, including ultrasounds, abdominal X Rays (AXR), CT scans and contrast studies.
Results
As seen in figure 1, the 41- 60 age group was the most susceptible to constipation, with the medical factors being the commonest cause, followed by medications.
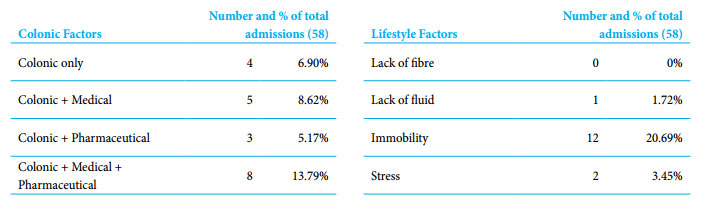
Relevant findings from table 1 include a high prevalence of immobility and a low prevalence of a poor fibre diet and fluid intake. This highlights that such information is not sought during primary assessment or admission, making it difficult to give advice on discharge.
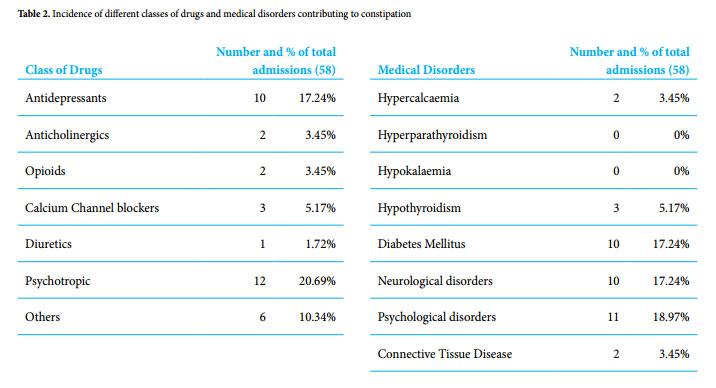
As shown in table 2 the low incidence of hypercalcaemia and the absence of hyperparathyroidism may be attributed to the fact that the calcium levels were not tested during admission. Only 6 out of 58 admissions (10.34%) were already on treatment for constipation.
As can be seen in figure 2, in total there were 19 patients who were admitted with colonic factors (one of whom was admitted twice), out of which only 4 had no other medical/ pharmaceutical contributing factors. Of the latter, only one had lifestyle factors (in this case stress) which possibly contributes to constipation. 15 out of these 19 patients had past abdominal surgery. 8 patients had past appendicectomies.

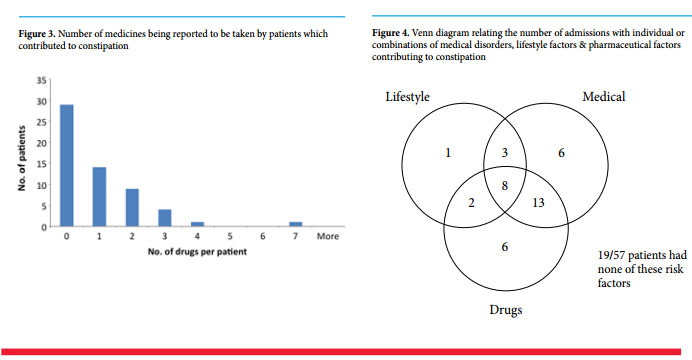
As seen in figure 3, of those patients who were not taking any medications (29 patients): • 16 had no risk factors (55.17%) – of which 10 were < 25 years old • 3 had only colonic factors (10.34%) • 3 had only medical factors (10.34%) • 3 had both medical and colonic factors (10.34%) • 1 had both medical and lifestyle factors (3.45%) • 2 had colonic, lifestyle and medical factors (6.90%)
Figure 4 is a Venn diagram representing the number of patients having one or more overlapping contributing lifestyle, medical or pharmaceutical factors. The most important observation from this Venn diagram is that it shows that the Class of Drugs Number and % of total admissions (58) Medical Disorders Number and % of total admissions (58) Antidepressants 10 17.24% Hypercalcaemia 2 3.45% Anticholinergics 2 3.45% Hyperparathyroidism 0 0% Opioids 2 3.45% Hypokalaemia 0 0% Calcium Channel blockers 3 5.17% Hypothyroidism 3 5.17% Diuretics 1 1.72% Diabetes Mellitus 10 17.24% Psychotropic 12 20.69% Neurological disorders 10 17.24% Others 6 10.34% Psychological disorders 11 18.97% Connective Tissue Disease 2 3.45% majority of patients admitted with constipation were already under medical care.
Conclusion
The GGH study showed that the predominant age group of those admitted because of constipation was between 41 and 60 years, followed closely by those between 61 and 80 years. In addition to this, the commonest factors contributing to constipation were noted to be medical conditions and regular medications. This shows that the patients who constituted the highest risk are those who are being treated by professionals, thus suggesting that management of constipation should be improved. A high incidence of past appendicectomies in admissions for constipation was also an interesting finding in Figure 3. Number of medicines being reported to be taken by patients which contributed to constipation 1 3 8 6 6 2 13 Lifestyle Medical Drugs 19/57 patients had none of these risk factors Figure 4. Venn diagram relating the number of admissions with individual or combinations of medical disorders, lifestyle factors & pharmaceutical factors contributing to constipation 10 our study, however, no related literature could be found, and so, it was concluded that this is an incidental finding since it is a common surgical procedure. During the data collection it was noted that sometimes history-taking, discharge advice and investigations were not thorough enough. Frequently, dietary habits and the mobility status were not noted in detail except in cases where it was obvious that the patients were bed-bound. Few were the cases in which dietary habits were recorded in files. The latter is especially important in elderly patients who may live alone and do not cook for themselves, and also for those patients with neurological deficits such as stroke and cerebral palsy who have special diets and difficulty in feeding.
All these issues need to be addressed and managed better. If the management is improved, the rate of admissions for constipation can be decreased. In view of this, following the study, a check-list was devised which was targeted at documentation and consideration of all factors discussed. A meeting with GPs in Gozo was also held where the data arising from the study was presented and the check-list explained. The importance of correctly filling this check list for patients was discussed with a view to help decrease the amount of admissions to hospital. The check-list may be accessed on www.thesynapse.com.
Acknowledgements
We would like to thank the staff of Gozo General Hospital, especially Mr Salvu Azzopardi and the staff of the records office for their help.