
Imaging Urinary Stone Disease: New Concepts
by Pierre Vassallo
Urinary stone disease is a universal problem that is particularly common in countries with warm climates like Malta and even more so during the hot summer months. It has been estimated that 14% of men and 6% of women suffer from urinary stone disease within their lifetime. In addition, many individuals will have recurrence of stone disease with stones recurring in 50% of cases within 5-10 years and 70% within 20 years. Over the last decade, an increase in stone disease in women has been reported.
Imaging urolithiasis (i.e. urinary tract stones) has evolved over the years due to technologic advances and a better understanding of the disease process. Baseline tests such as X-ray intravenous urography (IVU) have been replaced by computed tomography (CT), which resulted in improved diagnostic accuracy and speed and has avoided the need for bowel preparation and intravenous injection of contrast material (Figures 1 & 2). The efficiency of CT in detecting stones and monitoring treatment and follow-up has further improved with the development of spiral and multidetector technology and may offer further advantages with the introduction of Dual-Energy CT scanners. Sensitivity of CT for urinary tract stone detection is 95-98% with a specificity of 96-100%. CT also provides information regarding stone burden, composition, and fragility, all of which may aid in the selection of treatment strategies and may help in predicting success of treatment. In addition, CT detects extraurinary disease (that may mimic stone disease) such as appendicitis, diverticulitis, pancreatitis and gynaecological disorders. Other possible concurrent urinary tract diseases are also detectible with CT including renal abscesses, congenital anomalies and neoplasms, which could potentially alter the therapeutic approach.
As indicated earlier, the incidence of stone disease is strongly influenced by environmental factors, but dietary and genetic factors and certain chronic systemic diseases also play a role. Most stones (70-80%) are calcium-containing and include calcium oxalate monohydrate, calcium oxalate dehydrate and calcium phosphate. Stuvite stones account for 5-15% and are composed of magnesium ammonium phosphate. 5-10% of stones are uric acid stones, which occur in acid urine (pH <4.8) and may be treated by urinary alkalinisation. Cystine, xanthine and protein-matrix stones are usually due to hereditary factors, while drug stones are due to concentration of medication within the urine – such medications include Indavir, an antiretroviral agent used for HIV/AIDS treatment and Triamterene, a potassium-sparing diuretic. Indavir stones are not visualized by CT due to their low density, but clinical history should point towards this diagnosis. Hereditary and drug stones account for <5% of all stone disease.
Treatment of urinary tract stones depends on the patient’s symptoms and stone location, size and composition. Asymptomatic stones measuring <1cm in diameter are usually observed, as they are likely to pass spontaneously. Symptomatic stones of this size are treated with ureteronephroscopy or extracorporeal shockwave lithotripsy (ESWL), the former is particularly useful for low lying stones and the latter for stones in the renal pelvis or calyces. If fever occurs (i.e. secondary infection), a ureteric stent is inserted to relieve the kidney, and the stone may pass spontaneously or be extracted at a later date. Stones measuring 1-2cm in diameter may be treated with ESWL or percutaneous nephrolithotomy (PCNL). PCNL is an imaging-guided procedure that uses ultrasound or X-ray fluoroscopy to locate the stone and to guide puncture followed by dilatation of the tract through which the stone can be fragmented and extracted. While larger stones such as staghorn calculi may be treated by PCNL or laparoscopic or open nephrolithotomy.
Success of ESWL is related to a number of factors that may be evaluated with CT, including stone location (i.e. lower renal pole calyces versus other calices), size, and composition, as well as stone-to-skin distance. Ureteronephroscopy is an endoscopic procedure in which thin endoscopes (7-9 French in calibre) are inserted via the urethra and bladder into the ureter and renal pelvis. This procedure may be combined with laser and electrohydrolic or pneumatic lithotrites to shatter the stone and therefore ease its passage down the ureter.
Stone size and location are therefore the key factors that influence therapeutic planning of upper urinary tract stones. Stone composition also influences the choice of treatment. Cystine stones do not respond to ESWL and will require treatment with ureteronephroscopy or PCNL. Based on stone density, CT can distinguish three types of stone; Stones with a density < 400HU (Hounsfield Units) are likely to be uric acid stones and may be treated by oral dissolution therapy if asymptomatic. If symptomatic or causing obstruction, ESWL or ureteronephroscopy will be required. Stone with densities >400HU are classified as non-uric acid stones and are divided into two groups, those with densities <1000HU and those with readings > 1000HU. Those stones with densities 400-1000HU that are not cystine stones may be treated with ESWL and if refractory to that treatment with ureteronephroscopy or PCNL is administered depending on stone location. Those stones with densities >1000HU or cystine stones will require ureteronephroscopy or PCNL depending on location.
The most obvious CT sign of a urinary tract stone is naturally seeing the stone itself, however there are secondary signs that would improve detection rate particularly for matrix stones such as Indavir stones that have density readings similar to soft tissue (15-30HU). Secondary signs include perinephric and periureteric fat stranding, pelvic ureteric dilatation, periureteric oedema and unilateral renal enlargement (Figure 3). Stones <1cm in diameter that are accompanied by the presence of secondary signs are more likely to eventually require intervention with ureteronephroscopic extraction or lithotripsy. Intravenous contrast material may be used to identify the location of a non-CT-opaque stone, which would appear a filling defect in the contrast filled uretero-pelvi-calyceal system.
Stone burden influences the success of treatment and various ways of estimating stone size and volume on CT have been devised including linear and volumetric measurements as well as automated electronic volume estimation. It has been shown that a stone burden of more than 700 mm3 as determined from the product of the three spatial dimensions is a significant predictor of failure for ESWL.
Stone fragility can also be assessed by CT; a stone with heterogenous internal structure is likely to require less sessions and is more likely to respond to ESWL than stones with a homogeneous internal structure (Figure 4).
Stone composition has been shown to be reliably identified by CT in vitro. The attenuation values of urinary calculi usually fall within certain ranges: uric acid, 200–450 HU; struvite, 600–900 HU; cystine, 600–1100 HU; calcium phosphate, 1200–1600 HU; and calcium oxalate monohydrate, 1700–2800 HU. However measurement in vivo is not as reliable, and by general consensus CT density measurement is limited to the distinction of uric acid (<400HU) from non-uric acid (>400HU) stones and in the latter group, ESWL treatable (<1000HU) from less likely ESWL treatable (>1000HU) stones.
Dual-energy CT utilizes two X-ray beam energies (80 and 120kVp) to acquire tissue density information and through X-ray beam absorption of urinary tract stones is able to reliably distinguish calcium-containing from uric acid stones with a colour-coding for ease of diagnosis (Figure 5).
Location of a renal stone is also very important in planning therapy. A skin-to-stone distance (SSD) of >10cm indicates an increased likelihood of failure of potential treatment with ESWL. In addition, localization of the stone in the upper, mid or lower calyces will influence the percutaneous approach for PCNL.
CT analysis is finally useful for post-therapeutic assessment and important factors include, confirmation of stone-free status, assessment of residual stones and detection of residual renal obstruction, perirenal haematomas or urinomas. For dense stones larger than 10mm, plain X-rays may suffice to monitor stone position and state of fragmentation. After urologic intervention, identification of residual stones is important because the recurrence rates are higher with persistent stone fragments (50%–80%) than under stone-free conditions (10%–15%).
Despite the immense benefits of CT, there is some concern regarding its use in stone disease due to the risk of radiation exposure. This is particularly true in young individuals who undergo repeated CT examinations for stone disease and are consequently likely to be at risk for greater cumulative lifetime exposure. Rough estimates of radiation exposure in relation to the older and less sensitive IVU show a 2-5 fold increase. However careful selection of imaging parameters, limitation of scanned levels to the area-of-interest and new image processing alogrithms have resulted in a much reduced radiation exposure requirement for urologic CT (Figure 6).
In summary, CT currently plays an important management role in patients with urolithiasis, from the initial diagnosis to treatment planning and post-treatment follow-up. Keeping abreast of recent technologic developments helps to meet the growing expectations in this field. In addition, we must be aware of the radiation risk and to take appropriate measures to minimize this risk and optimize the diagnostic value of the technique.
Figure Legends

Fig 1. Axial CT scan showing a 4-mm stone in the left distal ureter (arrow).
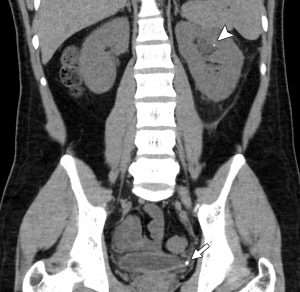
Fig 2. Coronal reformatted CT image shows the left distal ureteric stone (arrow) and a 2-mm stone in the left upper pole (arrowhead).

Fig 3. Axial CT scan reveals secondary signs of ureterolithiasis, including right renal enlargement, hydronephrosis (arrow), and perinephric stranding (arrowhead).
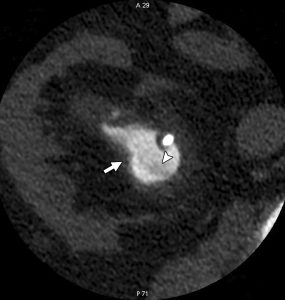
Fig 4. Axial CT scan in bone window settings shows internal inhomogeneities (arrowhead) within a stone (arrow) located in the right kidney.
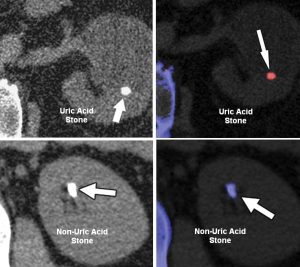
Fig 5. Dual-energy CT can reliably distinguish uric acid (coded red) from calcium-containing (coded blue) stones based on tissue attenuation characteristics.
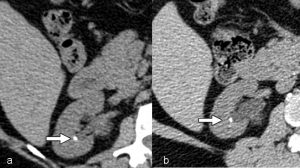
Fig 6. CT scans taken with normal (120kVp, 240mAs) (a) and with low-dose (100kVp, 100mAs) (b) settings, both allow confident diagnosis of the renal stone (arrow) in spite of graininess in the low dose image.