
Breast Cancer: Ductal Carcinoma in situ (DCIS)
by Pierre Vassallo
Ductal carcinoma in situ (DCIS) is a breast malignancy that is characterized by the proliferation of malignant ductal epithelial cells without evidence of invasion through the basement membrane. The incidence of DCIS has risen 11-fold between 1981 and 2001 through improved detection rates with screening mammography.
DCIS is not a single entity but a spectrum of disease ranging from low to high grade. DCIS grade is an important prognostic factor with high grade lesions being more likely to recur.
The simplest, most reproducible classification system of DCIS is the Van Nuys system, which identifies three groups of DCIS lesions. In the Van Nuys system, lesions are differentiated first according to nuclear grade (high, intermediate or low grade) and then according to whether necrosis is present or absent. Low-grade lesions contain cells with small nuclei, minimal nuclear pleomorphism, and infrequent mitoses, whereas high-grade lesions have cells with large, pleomorphic nuclei and frequent mitoses. Intermediate-grade lesions contain cells with nuclei that are neither low nor high grade. Figure 1 shows the Van Nuys system for classification of DCIS: First, lesions are classified according to whether they are of a high nuclear grade (group 3) or not. Non–high-grade lesions are further differentiated according to whether necrosis is present (group 2) or absent (group 1).
Mammography is the primary tool for detecting DCIS, but it has limitations. The reported sensitivity of mammography for detection of DCIS is between 87% and 95%. Mammography is more reliable in detecting higher grade lesions, while ultrasound was more useful than mammography for lower grade DCIS.
The most common mammographic finding in DCIS is microcalcifications. Microcalcifications tend to correlate with intraductal foci of necrosis. Thus a low-grade lesion without necrosis is less likely to manifest with calcifications than either an intermediate- or a high-grade lesion. Other mammographic findings might include a mass (Figure 2) or architectural distortion (Figure 3) and may be present in any grade lesion. The mass lesion in DCIS may directly correlate with tumor tissue, but may also be the result of periductal fibrosis or elastosis.
The most typical calcifications in DCIS are linear with or without branching (following the ducts) (Figure 4). Fragmentation of the calcifications is also indicative of malignancy, while rounded calcifications if abundant (>5 calcifications within an area 1cm in diameter) may also suggest DCIS (Figure 5).
Magnetic resonance (MR) imaging has higher sensitivity than mammography for the detection of DCIS and greater accuracy for depicting the extent of disease. However fibrocystic change may be indistinguishable and this leads to a poor specificity and also a limited usefulness of MRI for pre-operative planning. The MR appearance of DCIS depends primarily on the presence and extent of abnormal vascularity (tumor angiogenesis) resulting in the presence of abundant and leaky vessels. Therefore contrast-enhanced T1 weighted images are required that are obtained preferably as a 3D acquisition with high spatial resolution in a sequentially repeated fashion in order to observe both the degree and distribution of contrast agent uptake and the temporal the pattern of enhancement.
Non-mass-like (not nodule-shaped) enhancement typically involving a segment of the breast with some clumping is suggestive of DCIS (Figure 6). The kinetic pattern of contrast enhancement is more related to histologic grade with low grade lesions showing rapid uptake and loss of contrast material during the later phases (washout), whilst higher grade lesions tend to have slower uptake patterns with a prolonged plateau enhancement (Figure 7). Speed of contrast material uptake is related to vessel abundance, while the degree of prolongation of uptake (length of plateau phase) is a function of vessel permeability (leakiness).
The reported sensitivity of CT for the detection of DCIS ranges from 70% to 88%. In a different study, the detectability of the intraductal component of invasive ductal carcinomas at multidetector CT was compared with that at MR imaging; lesion detectability at multidetector CT was inferior to that at MR imaging. In general, CT has lower sensitivity but higher specificity than MR imaging because the lesion appearance leads to overestimation of fibrocystic changes at MR imaging. Multidetector CT may be used to map lesions for breast-conserving surgery, however presurgical mapping has been shown to be more helpful in invasive ductal cancers than for DCIS.
In summary, the incidence of DCIS has increased dramatically due to increased detection with screening mammography. The definitive correlation of histologic grading of DCIS (Van Nuys Classification) with mammographic findings and the use of MRI particularly in equivocal cases confirms the validity of both investigations, which can therefore strongly contribute to improved patient outcome.
Figure legends:
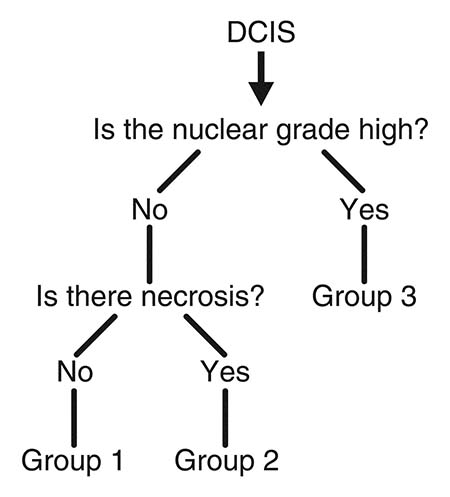
Figure 1. Van Nuys Classification
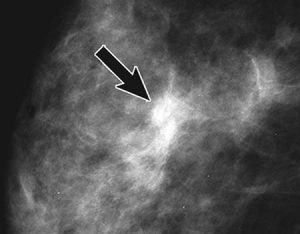
Figure 2. Mass lesion (arrow) in DCIS Grade 1
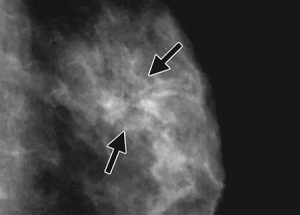
Figure 3. Architectural distortion (arrow) in DCIS Grade 1
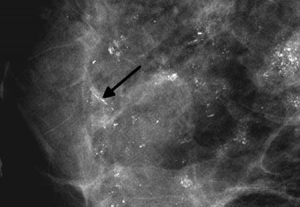
Figure 4. Linear calcifications in DCIS Grade 3
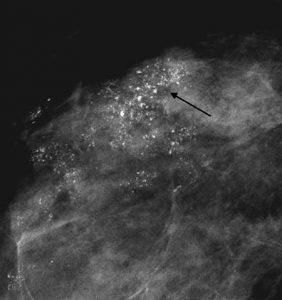
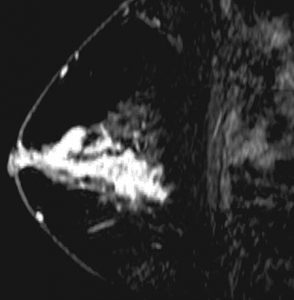
Figure 6. Segmental enhancement on MRI in DCIS Grade 3
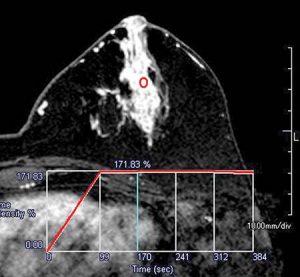
Figure 7. Kinetic analysis of contrast material uptake on MRI in Grade 3 DCIS: graph plotting degree of enhancement vs time shows rapid initial uptake and a prolonged plateau of enhancement