
COVID-19 Update on Facts and Imaging
Dr Pierre Vassallo
Since Dec 31, 2019, we have been bombarded by daily reports in the global news on the progress of spread of the Novel Corona Virus 2019, now known as COVID-19. While the information was worrying, a report issued by the Maltese Department of Health on March 7, 2020 confirmed that COVID-19 has finally hit home.1 At the time of submission of this article, Malta has three new cases of COVID-19 infection; all cases detected were from one Italian family residing in Malta, and all had returned from Northern Italy in the previous 2 weeks. Fortunately, all cases detected were already in quarantine at the time of detection.
Facts
Coronaviruses have a predilection for the respiratory tract. Numerous strains of the coronavirus exist, which can cause anything from the common cold to life-threatening respiratory infections. The disease is transmitted by a droplet mechanism (sneezing and coughing), hand contact (if hands are contaminated by sneezing or coughing) or by physical contact with an infected individual.
If COVID-19 virus remains within the upper respiratory tract, the presenting symptoms are those of the common cold (cough, sneezing and fever). If the virus involves the lower respiratory tract, it causes pneumonia, which can be severe and sometimes life-threatening particularly in elderly individuals and in those people whose immunity has been compromised by other diseases.
The main problem with controlling the disease is its incubation period of up to 14 days, during which time the individual carries the virus and can infect others but shows no symptoms. The present strategy for preventing spread is to enforce a 2-week self-quarantine (at home) on all those individuals returning from those regions with large numbers of infected cases; these include Northern Italy, China, Singapore, Japan, Iran and South Korea.
The media have undoubtedly had a major impact on the level of awareness of this disease worldwide. It is impressive to see reports from reliable sources such as the European Centre for Disease Prevention and Control, where in almost real-time, we learn of the number of cases in each country. It is rather disturbing, as of March 7, to see large countries such as Ukraine and Bhutan, which have one case each,2 while Malta has three. However, these reports must be evaluated with caution, because the quality of the national health services in each country will impact the number of detected and reported cases. On a more critical note, it would be interesting to see how statistics for other viruses (such as the influenza virus) compare with those of COVID-19 to understand whether this is really a new scenario or just another “déjà vu”.
Diagnostic Criteria
One of the first peer-reviewed scientific publications that reported on the signs and symptoms of Coronavirus appeared in the New England Journal of Medicine on January 29, 2020.3 This article reported on clinical findings in the first 425 recorded cases of COVID-19 from Wuhan, Hubei Provence, China. These were confirmed using real-time Reverse Transcription Polymerase Chain Reaction (RT-PCR) performed on swabs taken from the upper respiratory tract or from bronchial lavage samples. Initially, only symptomatic cases who had direct or indirect contact with the Wuhan Seafood Market were tested. Subsequently, test criteria were updated and a sharp rise in the number of confirmed cases was observed with a marked increase in non-linked cases.3 Due to the limited resources for RNA testing in China resulting from the large demand, health authorities were obliged to introduce clinical and imaging findings as well as a history of exposure as criteria for diagnosing COVID-19 infection in the Hubei Provence; this further complicated statistical evaluation, making the effects of disease containment measures more difficult to assess.4,5
Clinical Presentation
A report from the Chinese Centre for Disease Control has shown that most case patients were 30 to 79 years of age (87%), 1% were aged 9 years or younger, 1% were aged 10 to 19 years, and 3% were age 80 years or older.4 In this report, most cases had been diagnosed in Hubei Province (75%) and many of those reported Wuhan-related exposures (86%).
Most cases were classified as mild (81%; i.e. nonpneumonia and mild pneumonia). However, 14% were severe (i.e. dyspnea, respiratory frequency ≥30/min, blood oxygen saturation ≤93%, partial pressure of arterial oxygen to fraction of inspired oxygen ratio <300, and/or lung infiltrates >50% within 24 to 48 hours), and 5% were critical (i.e. respiratory failure, septic shock, and/or multiple organ dysfunction or failure).5
Imaging Findings
The most valuable method for imaging COVID-19 infection is chest CT (computed tomography). Most affected patients have shown the following CT findings:
- Ground glass opacities (GGO)
- Mixed GGO and lung consolidation
- Vascular enlargement and
- Traction bronchiectasis.
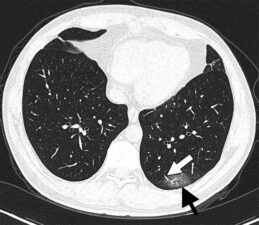
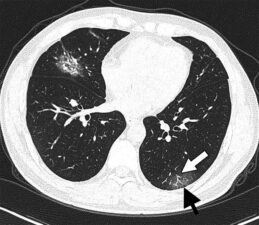
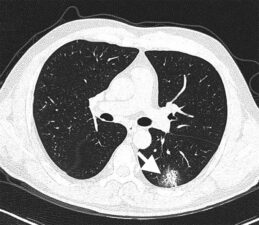
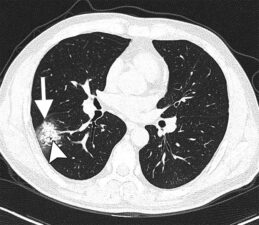
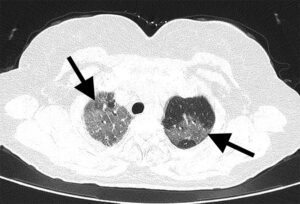
Figure 1 illustrates the above CT findings in a patient who had a short-term exposure to Wuhan and was suffering from fever and cough; these clinic features are considered as mild symptoms.6
Lung lesions in COVID-19 infection are more likely to be bilateral, basal, multifocal and peripheral.
Two reports have shown that patients showing the following lung CT findings are more likely to already have or to progress to severe life-threatening disease:6,7
- Architectural distortion
- Traction bronchiectasis
- Lymph node enlargement and
- Pleural effusions.
Finally, one research group indicated that diffuse lung disease is more frequent in severe cases.6
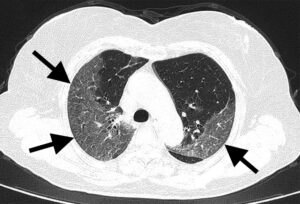
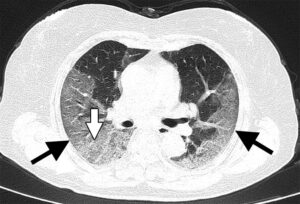
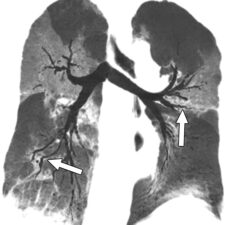
Figures 2 and 3 illustrate some of the above features in patients with confirmed COVID-19 infection who were suffering from severe symptoms including respiratory distress. These findings may be seen in any severe lower respiratory tract infection.
In summary, even though the above CT scan features may not be pathognomonic for COVID-19 infection, they are useful in detecting RT-PCR negative or equivocal cases and in the absence of lab resources as was experienced in China when demand outstripped the supply for testing kits. CT may also be useful in detecting subclinical infections. Based on the above report, CT is helpful for identifying those cases that have or are likely to progress to severe life-threatening disease.
Figure legends:
Figure 1: CT images show bilateral multifocal ground-glass opacities (GGO) (black arrows in a and b), mixed GGO (white arrow in c) and consolidation lesions (arrow in d). Traction bronchiectasis (arrowhead, d) and vascular enlargement (white arrow, a and b) are also noted.
Figure 2: CT Scans through the lungs (a, b and c) show bilateral diffuse ground glass opacities (black arrows in a, b and c) and reticulation (white arrow in c).
Figure 3: Coronal CT reconstruction show irregular bronchial wall with traction bronchiectasis and architectural distortion (white arrows).
References
- Novel Coronavirus. Dept of Health, Malta, 07-Mar-2020. Online. Available: https://deputyprimeminister.gov.mt/en/health-promotion/Pages/Novel-coronavirus.aspx. Accessed: 07 Mar 2020.
- Situation update worldwide, as of 7 March 2020 08: 00. European Centre for Disease Prevention and Control, 07-Mar-2020. Online. Available: https://www.ecdc.europa.eu/en/geographical-distribution-2019-ncov-cases. Accessed: 07 Mar 2020.
- Li Q, Guan X, Wu P et al. Early Transmission Dynamics in Wuhan, China, of Novel Coronavirus–Infected Pneumonia. NEJM 2020. Epub ahead of print. Available from: https://www.nejm.org/doi/10.1056/NEJMoa2001316?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub%3dwww.ncbi.nlm.nih.gov
- The Novel Coronavirus Pneumonia Emergency Response Epidemiology Team. The Epidemiological Characteristics of an Outbreak of 2019 Novel Coronavirus Diseases (COVID-19). China CDC Weekly 2020; 2(8):113-122
- Wu Z, McGoogan JM. Characteristics of and Important Lessons From theCoronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72 314 Cases From the Chinese Center for Disease Control and Prevention. JAMA 2020. Epub ahead of print. Available from: https://jamanetwork.com/journals/jama/fullarticle/2762130
- Zhao W, Zhong Z, Xie X, et al. Relation Between Chest CT Findings and Clinical Conditions of Coronavirus Disease (COVID-19) Pneumonia: A Multicenter Study. American Journal of Roentgenology 2020; 215: 1-6. Epub ahead of print. Available from: https://www.ajronline.org/doi/full/10.2214/AJR.20.22976
- Li Y, Xia L. Coronavirus Disease 2019 (COVID-19): Role of Chest CT in Diagnosis and Management. American Journal of Roentgenology 2020. Epub ahead of print. Available from: https://www.ajronline.org/doi/full/10.2214/AJR.20.22954